
By Shifaa Qaqa T wo bulky lateral lobes Isthmus Follicles Follicular epithelial cells TSH Thyroglobulin T4 T3 bound to circulating plasma proteins The interaction of thyroid hormone with its nuclear thyroid hormone receptor TR results in the formation of a h ID: 909070
Download Presentation The PPT/PDF document "Pathology of the thyroid gland" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

Slide1
Pathology of the thyroid gland
By :
Shifaa
’
Qa’qa
’
Slide2T
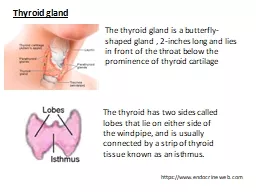
wo bulky lateral lobes
Isthmus
Follicles
Follicular epithelial cells
TSH
Thyroglobulin ---- T4 , T3 ---- bound to circulating plasma proteins
Slide3Slide4The interaction of thyroid hormone with its nuclear thyroid hormone receptor (TR) results in the formation of a hormone-receptor complex that binds to
thyroid hormone response elements (TREs) in target genes
, regulating their transcription.
Slide5Hyperthyroidism
Hypothyroidism
Slide6HYPERTHYROIDISM
Thyrotoxicosis
:
Elevated circulating levels of free T3 and T4
Hyperthyroidism is mc
Slide7Slide8Manifestations of thyrotoxicosis:
Hypermetabolic
state
heat intolerance
weight loss
despite increased appetite
soft, warm, and flushed skin
malabsorption
, and
diarrhea
Palpitations and tachycardia
congestive heart failure
nervousness,
tremor
, and irritability
50% develop proximal muscle weakness (thyroid myopathy)
Slide9staring gaze and lid lag (
sympathetic overstimulation of the
levator
palpebrae
superioris
)
True thyroid
ophthalmopathy
associated with
proptosis
/
exophthalmus
is a feature seen only in
Graves disease ----
Bilateral, accumulation of
loose
connective tissue, fatty infiltration, mononuclear cells infiltration, and edema
behind the orbits---- corneal damage
Slide10Thyroid storm:
Hyperthyroidism patient ---- stress (
truama
, surgery, emotional, infection,)
---- not receive
Tx
medical emergency
Tachycardia, cardiac arrhythmias (AF), fever, agitation, confusion
Slide11Apathetic hyperthyroidism--- elderly persons
Slide12The measurement of serum TSH is the most useful single screening test for hyperthyroidism
- TSH levels are decreased, increased levels of
free T4 or occasionally free T3
- TSH levels normal or raised ; pituitary- or hypothalamus-associated (secondary) hyperthyroidism
Slide13measurement of radioactive iodine uptake by the thyroid gland often is valuable in determining the etiology
.
such scans may show diffusely increased (whole gland) uptake in Graves disease
increased uptake in a solitary nodule in toxic adenoma
decreased uptake in thyroiditis.
Slide14HYPOTHYROIDISM
Worldwide, the most common cause of hypothyroidism is dietary deficiency of iodine ,
while in most developed nations, autoimmune causes predominate.
Slide15Slide16Manifestations:
Cretinism
Slide17Slide18Myxedema
:
Gull disease
Generalized apathy
mental sluggishness
cold intolerant
Obese
constipation
coarsening of facial features, enlargement of the tongue, and deepening of the voice (accumulation of
m
ucopolysaccharide
-rich edematous fluid)
heart failure
Slide19Slide20measurement of serum TSH is the most sensitive screening test
serum TSH--increased--- primary hypothyroidism
serum TSH—not increased--- secondary
hypothy
Serum T4--- decreased
Slide21THYROIDITIS
inflammation of the thyroid
(1) Hashimoto thyroiditis
(2) granulomatous (de
Quervain
) thyroiditis;
(3)
subacute
lymphocytic thyroiditis
Slide22Hashimoto thyroiditis
:
the mc cause of hypothyroidism in areas of the world where iodine levels are sufficient.
it may be preceded by transient thyrotoxicosis
Chronic Lymphocytic Thyroiditis
45 and 65 years, Females, painless enlargement of the thyroid,
Autoimmune--- other autoimmune diseases
increased risk for the development of B cell non-Hodgkin lymphomas and papillary carcinomas
Slide23Slide24antithyroid
antibodies:
antithyroglobulin
,
antithyroid
peroxidase antibodies
The thyroid usually is
diffusely
and
symmetrically
enlarged
Slide25Slide26Subacute
Lymphocytic Thyroiditis
:
in a subset of patients the onset of disease follows pregnancy (
postpartum thyroiditis
)
Autoimmune, females
painless neck mass
Thyrotoxicosis ---
euthyroid
--- hypothyroidism
Slide27Subacute
Granulomatous
(de
Quervain
)
Thyroiditis
:
ages of 30 and 50
Females
Viral infection—
hx
of an upper respiratory infection
pain in the neck, fever, malaise
Transient hyperthyroidism--- transient
Hypothyroidism
self-limited
----
euthyroid
state within 6 to 8 weeks.
Slide28Riedel thyroiditis
:
extensive
fibrosis
involving the thyroid and contiguous neck structures
fixed thyroid mass, simulating a thyroid neoplasm.
autoimmune
Slide29GRAVES DISEASE
Graves disease is the most common cause of endogenous hyperthyroidism
Triad of:
1- Thyrotoxicosis (diffusely enlarged thyroid)
2-
Ophthalmopathy
---- exophthalmos
3-
dermopathy
/ pretibial myxedema/ shins (
glycosaminoglycans
and lymphocyte infiltration)
ages of 20 and 40, females, autoimmune
Slide30breakdown in self-tolerance to thyroid
autoantigens
, of which the most important is the
TSH receptor.
Thyroid-stimulating immunoglobulin
Thyroid growth-stimulating
immunoglobulins
TSH-binding inhibitor
immunoglobulins
T cell–mediated-----
ophthalmopathy
Slide31The thyroid gland is enlarged, symmetrically
diffuse
Slide32Slide33DIFFUSE AND MULTINODULAR
GOITER
impaired synthesis of thyroid hormone (dietary iodine deficiency)
--------------
compensatory rise in the serum TSH, which in turn causes hypertrophy and hyperplasia of thyroid follicular cells
---------------
Goiter : Enlargement of the thyroid ----- large neck mass---- airway obstruction, dysphagia, and compression of large vessels in the neck and upper thorax
(so-called superior
vena cava syndrome).
---------------------
enough to overcome the hormone deficiency, ensuring a
euthyroid
metabolic state
Slide34Endemic goiter------- little iodine
Sporadic goiter----- physiologic demand for T4, puberty, females
Slide35D
iffuse goiter ---- diffuse, symmetric enlargement of the gland
recurrent episodes of hyperplasia and involution
M
ultinodular
goiter ---- irregular enlargement
of the thyroid
toxic
multinodular
goiter ----- autonomous nodules ----Plummer syndrome