
Shehabat MSc PhD Consist of Four Nuclei striatum caudate and putamen globus pallidus substantia nigra subthalamus The basal ganglia are the principal subcortical components of a family of parallel ID: 910270
Download Presentation The PPT/PDF document "Basal Ganglia Mustafa Al-" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
Basal GangliaMustafa Al-Shehabat MSc, PhD
Consist of Four Nuclei
striatum
caudate and putamen
globus pallidus
substantia nigra
subthalamus
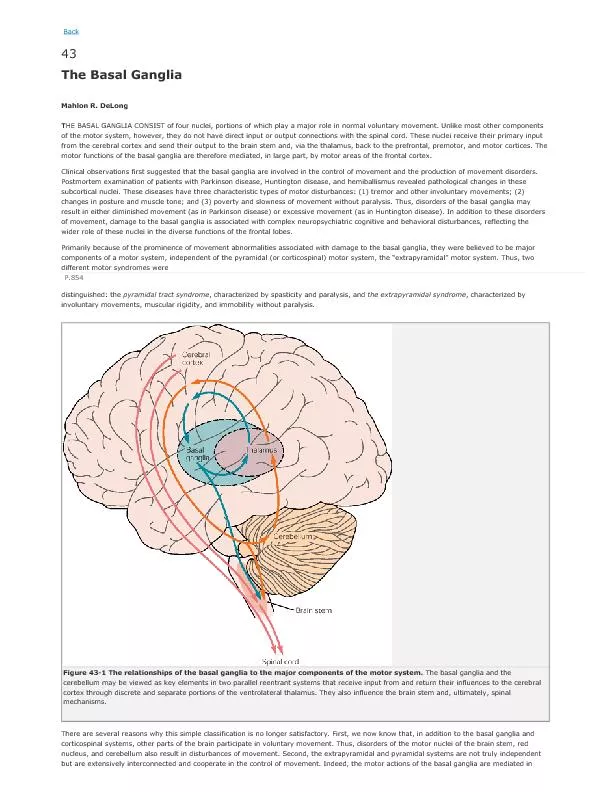
Slide2The basal ganglia are the principal subcortical components of a family of parallel circuits linking the thalamus with the cerebral
cortex
Slide3Motor Function of the Basal Gangliacontrol of complex patterns of motor activityusing scissorsthrowing balls
shoveling
dirt
Slide4Function of the Basal Ganglia?not much is known about the specific functions of each of these structuresthought to function in timing and scaling of motion and in the initiation of motionmost information comes from the result of damage to these structures and the resulting clinical abnormality
Slide5Caudate extends into all lobes of the cortex and receives a large input from association areas of the cortexMostly projects to globuspallidus, no fibers to sub-thalamus or substantia nigra
Most motor actions occur as a result of a sequence of thoughts. Caudate circuit may play a role in the cognitive control of motor functions
Caudate Circuit
Slide6Putamen CircuitMostly from premotor and supplemental motor cortex to putamen then back to motor cortex.
Slide7Neurotransmitters in the Basal Ganglia
Slide8Lesions of Basal Gangliaglobus pallidusathetosis - spontaneous writing movements of the hand, arm, neck, and faceputamenchorea - flicking movements of the hands, face, and shoulders
substantia nigra
Parkinson's disease - rigidity, tremor and akinesia
loss of dopaminergic input from substantia nigra to the caudate and putamen
Slide9subthalamushemiballismus - sudden flailing movements of the entire limbcaudate nucleus and putamenhuntington’s chorea - loss of GABA containing neurons to globus pallidus and substantia nigra
Lesions of Basal Ganglia
Slide10Integration of Motor Controlspinal cord levelpreprogramming of patterns of movement of all muscles (i.e., withdrawal reflex, walking movements, etc.).brainstem levelmaintains equilibrium by adjusting axial tone
cortical level
issues commands to set into motion the patterns available in the spinal cord
controls the intensity and modifies the timing
Slide11Integration of Motor Control (cont’d)cerebellum function with all levels of control to adjust cord motor activity, equilibrium, and planning of motor activitybasal ganglia functions to assist cortex in executing subconscious but learned patterns of movement, and to plan sequential patterns to accomplish a purposeful task
Slide12Overall scheme forintegration ofmotor function
Slide13History of Parkinson´s disease (PD)First described in 1817 by an English physician, James Parkinson, in “An Essay on the Shaking Palsy.”
The famous French neurologist, Charcot, further described the syndrome in the late 1800s.
Slide14Epidemiology of PDThe most common movement disorder affecting 1-2 % of the general population over the age of 65 years.
The second most common neurodegenerative disorder after Alzheimer´s disease (AD).
Slide15Incidence of PDAge
Incidence / 100 000
Slide16Prevalence of PDAge
Prevalence / 100 000
Slide17Epidemiology of PDMay be less prevalent in China and other Asian countries, and in African-Americans.Prevalence rates in men are slightly higher than in women; reason unknown, though a role for estrogen has been debated.
Slide18Risk factors of PDAge - the most important risk factor
Positive family history
Male gender
Environmental exposure: Herbicide and pesticide exposure, metals (manganese, iron), well water, farming, rural residence, wood pulp mills; and steel alloy industries
Race
Life experiences (trauma, emotional stress, personality traits such as shyness and depressiveness)?
An inverse correlation between cigarette smoking and caffeine intake in case-control studies.
Slide19Clinical features of PDThree cardinal features:® resting tremor® bradykinesia (generalized slowness of movements)
®
muscle rigidity
Slide20Clinical features of PDResting tremor: Most common first symptom, usually asymmetric and most evident in one hand with the arm at rest.
Bradykinesia:
Difficulty with daily activities such as writing, shaving, using a knife and fork, and opening buttons; decreased blinking, masked facies, slowed chewing and swallowing.
Rigidity:
Muscle tone increased in both flexor and extensor muscles providing a constant resistance to passive movements of the joints; stooped posture, anteroflexed head, and flexed knees and elbows.
Slide21Additional clinical features of PDPostural instability: Due to loss of postural reflexes.
Dysfunction of the autonomic nervous system: Impaired
gastrointestinal motility, bladder dysfunction, sialorrhea, excessive head and neck sweating, and orthostatic hypotension.
Depression: Mild to moderate depression in 50 % of patients.
Cognitive impairment: Mild cognitive decline including impaired visual-spatial perception and attention, slowness in execution of motor tasks, and impaired concentration in most patients; at least 1/3 become demented during the course of the disease.
Slide22Neuropathology of PDEosinophilic, round intracytoplasmic inclusions called lewy bodies and Lewy neurites.
First described in 1912 by a German neuropathologist - Friedrich Lewy.
Inclusions particularly numerous in the substantia nigra pars compacta
.
Slide23Lewy bodies
Slide24Neuropathology of PD: Lewy bodiesNot limited to substantia nigra only; also found in the locus coeruleus, motor nucleus of the vagus nerve, the hypothalamus, the nucleus basalis of Meynert, the cerebral cortex, the olfactory bulb and the autonomic nervous system.
Confined largely to neurons; glial cells only rarely affected.
Slide25Functional neuroanatomy of PDSubstantia nigra: The major origin of the dopaminergic innervation of the striatum.Part of extrapyramidal system which processes information coming from the cortex to the striatum, returning it back to the cortex through the thalamus.
One major function of the striatum is the regulation of posture and muscle tonus.
Slide26Neurochemistry of PD Late 1950s: Dopamine (DA) present in mammalian brain, and the levels highest within the striatum.
1960, Ehringer and Hornykiewicz: The levels of DA severely reduced in the striatum of PD patients.
PD symptoms become manifest when about 50-60 % of the DA-containing neurons in the substantia nigra and 70-80 % of striatal DA are lost.
Slide27Dopamine synthesis
Slide28Dopamine pathways in human brain
Slide29Therapy of PD: levodopaLate 1950s: L-dihydroxyphenylalanine (L-DOPA; levodopa), a precursor of DA that crosses the blood-brain barrier, could restore brain DA levels and motor functions in animals treated with catecholamine depleting drug (reserpine).First treatment attempts in PD patients with levodopa resulted in dramatic but short-term improvements; took years before it become an established and succesfull treatment.
Still today, levodopa cornerstone of PD treatment; virtually all the patients benefit.
Slide30Therapy of PD: limitations of levodopaEfficacy tends to decrease as the disease progresses.
Chronic treatment associated with adverse events (motor fluctuations, dyskinesias and neuropsychiatric problems).
Slide31Therapy of PD: limitations of levodopaDoes not prevent the continuous degeneration of nerve cells in the subtantia nigra, the treatment being therefore symptomatic.
Slide32Inhibition of peripheral COMT
by entacapone
increases the amount of L-DOPA and dopamine in the brain and
improves the alleviation of P
D
symptoms.
Slide33Therapy of PD: Other treatmentsDA receptor agonists (bromocriptine, pergolide, pramipexole, ropinirole, cabergoline)
Amantadine
Anticholinergics
Slide34Diagnosis of PD History and clinical examination Positron
Emission Tomography (PET) or Single-photon Emission Computed Tomography (SPECT) with dopaminergic radioligands
Exclusion of several causes of secondary Parkinsonism
Slide35Summary 1-2 % of the general population over the age of 65 yLewy bodies and Lewy neurites particularly in the substantia nigra pars compacta dopaminergic neurons projecting to striatum
DA levels severely reduced in striatum.
Resting tremor, bradykinesia, muscle rigidity
Levodopa and other dopaminergic drugs
No treatment which would prevent the continuous degeneration of nerve cells in the substantia nigra and resulting striatal DA loss