
Posttraumatic stress disorder PTSD constitutes a prevalent concern among individuals with cancer with prevalence ranging from 3 to 4 in earlystage cancer diagnosis to 35 in individuals following medical treatment ID: 1012414
Download Presentation The PPT/PDF document "OBJECTIVES RESULTS CONCLUSIONS" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






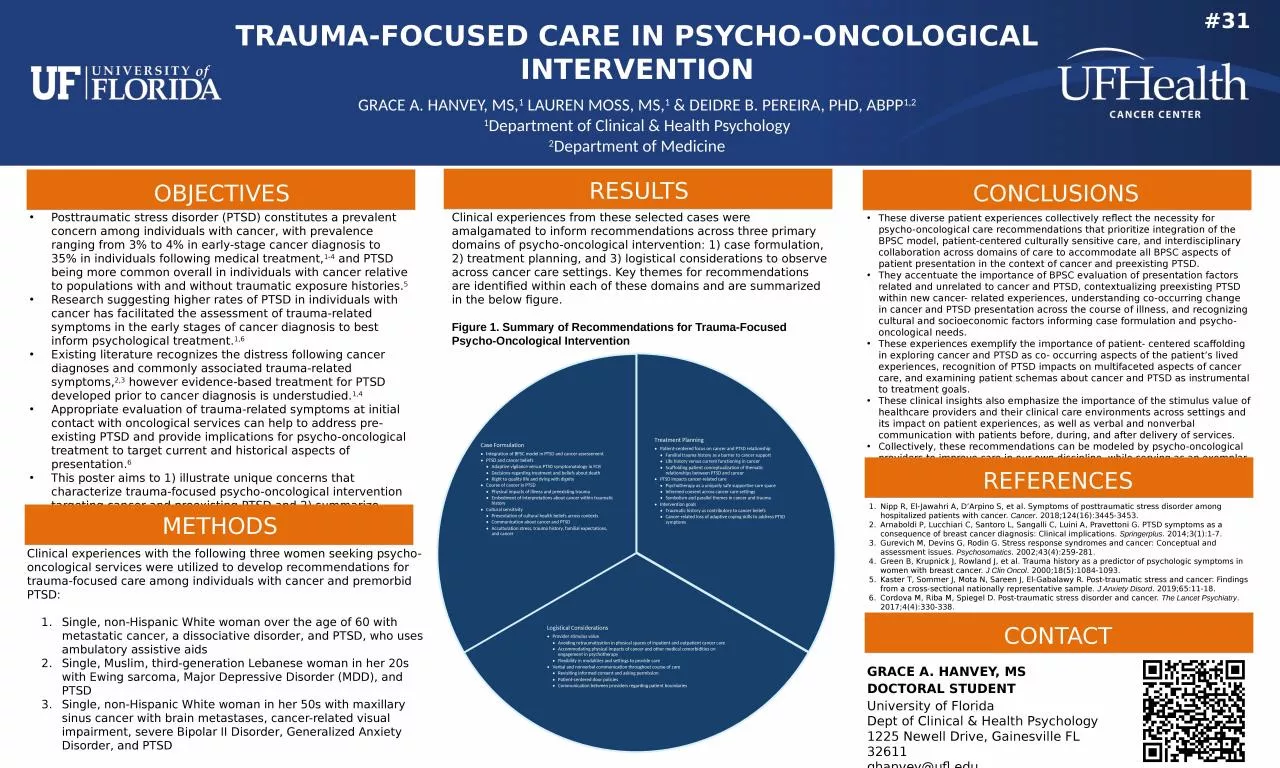
1. OBJECTIVESRESULTSCONCLUSIONSPosttraumatic stress disorder (PTSD) constitutes a prevalent concern among individuals with cancer, with prevalence ranging from 3% to 4% in early-stage cancer diagnosis to 35% in individuals following medical treatment,1-4 and PTSD being more common overall in individuals with cancer relative to populations with and without traumatic exposure histories.5 Research suggesting higher rates of PTSD in individuals with cancer has facilitated the assessment of trauma-related symptoms in the early stages of cancer diagnosis to best inform psychological treatment.1,6 Existing literature recognizes the distress following cancer diagnoses and commonly associated trauma-related symptoms,2,3 however evidence-based treatment for PTSD developed prior to cancer diagnosis is understudied.1,4 Appropriate evaluation of trauma-related symptoms at initial contact with oncological services can help to address pre-existing PTSD and provide implications for psycho-oncological treatment to target current and historical aspects of presentation.6 This poster aims to 1) illustrate unique concerns that characterize trauma-focused psycho-oncological intervention targeting cancer and preexisting PTSD and 2) summarize recommendations for providing care to these individuals across interdisciplinary cancer care teams. METHODSClinical experiences with the following three women seeking psycho-oncological services were utilized to develop recommendations for trauma-focused care among individuals with cancer and premorbid PTSD: Single, non-Hispanic White woman over the age of 60 with metastatic cancer, a dissociative disorder, and PTSD, who uses ambulatory assistive aids Single, Muslim, third-generation Lebanese woman in her 20s with Ewing sarcoma, Major Depressive Disorder (MDD), and PTSD Single, non-Hispanic White woman in her 50s with maxillary sinus cancer with brain metastases, cancer-related visual impairment, severe Bipolar II Disorder, Generalized Anxiety Disorder, and PTSD Overarching themes surrounding clinical experiences were qualitatively identified in reflection on clinical observations among the psycho-oncological providers of these women. These diverse patient experiences collectively reflect the necessity for psycho-oncological care recommendations that prioritize integration of the BPSC model, patient-centered culturally sensitive care, and interdisciplinary collaboration across domains of care to accommodate all BPSC aspects of patient presentation in the context of cancer and preexisting PTSD. They accentuate the importance of BPSC evaluation of presentation factors related and unrelated to cancer and PTSD, contextualizing preexisting PTSD within new cancer- related experiences, understanding co-occurring change in cancer and PTSD presentation across the course of illness, and recognizing cultural and socioeconomic factors informing case formulation and psycho-oncological needs. These experiences exemplify the importance of patient- centered scaffolding in exploring cancer and PTSD as co- occurring aspects of the patient’s lived experiences, recognition of PTSD impacts on multifaceted aspects of cancer care, and examining patient schemas about cancer and PTSD as instrumental to treatment goals. These clinical insights also emphasize the importance of the stimulus value of healthcare providers and their clinical care environments across settings and its impact on patient experiences, as well as verbal and nonverbal communication with patients before, during, and after delivery of services. Collectively, these recommendations can be modeled by psycho-oncological providers to improve care in our own discipline, while serving as an exemplar for optimizing care across inpatient and outpatient oncological services. REFERENCESNipp R, El-Jawahri A, D’Arpino S, et al. Symptoms of posttraumatic stress disorder among hospitalized patients with cancer. Cancer. 2018;124(16):3445-3453. Arnaboldi P, Lucchiari C, Santoro L, Sangalli C, Luini A, Pravettoni G. PTSD symptoms as a consequence of breast cancer diagnosis: Clinical implications. Springerplus. 2014;3(1):1-7. Gurevich M, Devins G, Rodin G. Stress response syndromes and cancer: Conceptual and assessment issues. Psychosomatics. 2002;43(4):259-281. Green B, Krupnick J, Rowland J, et al. Trauma history as a predictor of psychologic symptoms in women with breast cancer. J Clin Oncol. 2000;18(5):1084-1093. Kaster T, Sommer J, Mota N, Sareen J, El-Gabalawy R. Post-traumatic stress and cancer: Findings from a cross-sectional nationally representative sample. J Anxiety Disord. 2019;65:11-18. Cordova M, Riba M, Spiegel D. Post-traumatic stress disorder and cancer. The Lancet Psychiatry. 2017;4(4):330-338. CONTACTGRACE A. HANVEY, MSDOCTORAL STUDENTUniversity of FloridaDept of Clinical & Health Psychology1225 Newell Drive, Gainesville FL 32611ghanvey@ufl.eduQR CodeTRAUMA-FOCUSED CARE IN PSYCHO-ONCOLOGICAL INTERVENTIONGRACE A. HANVEY, MS,1 LAUREN MOSS, MS,1 & DEIDRE B. PEREIRA, PHD, ABPP1,21Department of Clinical & Health Psychology2Department of Medicine#31Clinical experiences from these selected cases were amalgamated to inform recommendations across three primary domains of psycho-oncological intervention: 1) case formulation, 2) treatment planning, and 3) logistical considerations to observe across cancer care settings. Key themes for recommendations are identified within each of these domains and are summarized in the below figure. Figure 1. Summary of Recommendations for Trauma-Focused Psycho-Oncological Intervention