

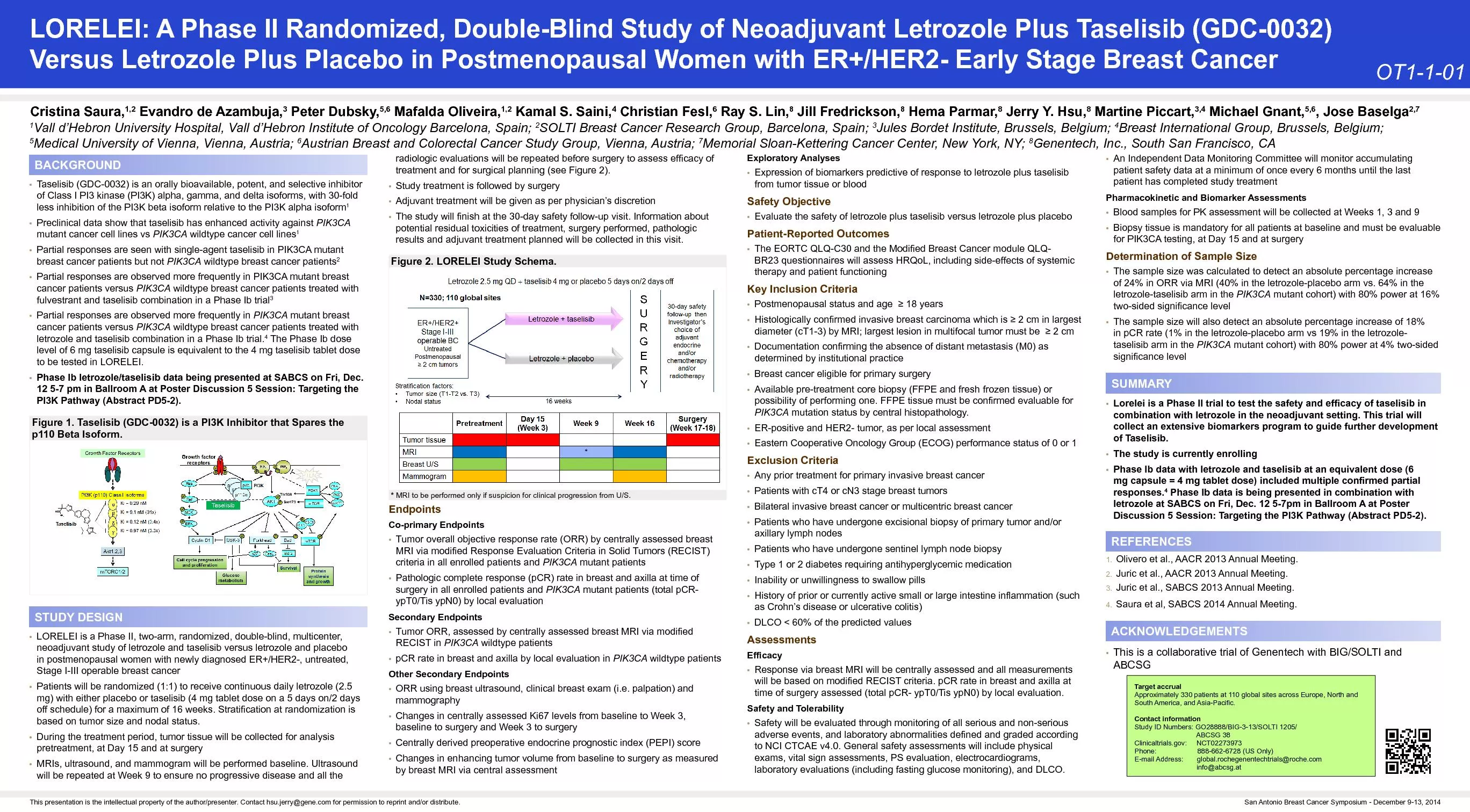
TNT SIMPLIFIED STAGING STAGE I NO LYMPH NODE SMALL TUMOR STAGE II NO LYMPH NODE INVADES SUBSEROSA STAGE III LYMPH NODES with cancer STAGE IV Distant METASTASIS FOCUS FOR TODAY IS STAGE II AND III RECTAL CANCER ID: 1033277
Download Presentation The PPT/PDF document "TOTAL NEOADJUVANT THERAPY" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



1. TOTAL NEOADJUVANT THERAPY TNT
2. SIMPLIFIED STAGINGSTAGE I NO LYMPH NODE, SMALL TUMORSTAGE II NO LYMPH NODE, INVADES SUBSEROSASTAGE III LYMPH NODES with cancerSTAGE IV Distant METASTASISFOCUS FOR TODAY IS STAGE II AND III RECTAL CANCER
3. DEFINITIONSNEOADJUVANT Rx - Rx given before the primary treatmentADJUVANT Rx - Rx given after primary treatment Targets cancer cells that the primary treatment may not have destroyedCLINICAL COMPLETE RESPONSE cCR No visible evidence of tumor in the rectum and mesorectal nodesPATHOLOGIC COMPLETE RESPONSE pCR No viable tumor in primary site/mesorectal lymph nodes in the resected surgical specimen
4. CASE83-year-old male diagnosed with stage III rectal cancer. Which of the following treatments would be potentially appropriate?SurgeryRadiation therapyChemotherapyImmunotherapy (FOR NON-STAGE IV DISEASE ??)
5. SURGERY First modality used Radical surgery, Hartman, anterior rectal resection High local recurrence rate > 30% High rate of distant metastases > 30%Total mesorectal excision (TME) 1986 Dramatic decrease in local recurrence rate, to 4 to 12% BUT distant metastases remained a major problem postop 25 to 30% of patients still developed distant metastatic disease
6. TOTAL MESORECTAL EXCISIONTME goal is complete removal of the rectum, together with the surrounding lymphovascular fatty tissue containing pararectal lymph nodes, preserve nerve fibers that supply the urinary bladder, prostate and vaginaINCORRECTCORRECT
7. RADIATION THERAPYQUESTION ?? Increase local control. See if that translates to better overall survivalInitial studies focused on postop adjuvant radiation therapy vs noneSignificant decrease in local recurrence noted No overall survival benefit noted.However, high rate of toxicity due to postoperative morbidityLed to the idea of preoperative (NEOADJUVANT) radiation therapy1985 GITSG 55/33
8. 1985 GITSGProlongation of the disease-free interval in surgically treated rectal carcinomaGastrointestinal Tumor Study Group Postop adjuvant therapy versus no adjuvant therapy.Adjuvant therapy consisting of radiation alone, chemotherapy alone, chemotherapy with radiation therapy. Basically 4 groups. Surgery alone was a control arm.Study was significant for finding as compared to surgery, adjuvant therapy decreased rates of local recurrence and improved disease-free survival. No overall survival seen.L LR 55% versus 33% for CRT. TME not the standard.DFI, significantly better with CRT Overall survival same. Note that the chemotherapy used was 5 FU with methyl CCNU. Methyl CCNU later found out not to add any benefit to 5-FU alone and was associated with significant toxicity and hence that was no longer used.The most profound effect was seen in postoperative chemotherapy with radiation therapy.
9. NEOADJUVANT RADIATION RxRATIONALEAdequate oxygen supply needed to the treated area for maximum radiation therapy benefit. Tissue hypoxia ? less DNA damage from radiation therapy to the treated area(cancer)Surgery causes disruption of blood supplyTheoretically, less oxygen delivered to postoperative site.Higher dose of radiation therapy needed to effectively kill microscopic diseaseHence, potentially more toxicity when radiation given post op.
10. NEOADJUVANT RADIATIONSwedish and Dutch studies 1997 and 2001Radiation before surgery versus surgery aloneSignificant decrease in local recurrence rate with preop RT. 11% versus 27%, 2% vs 8%Swedish study improved overall survival (TME not standard) 58% vs 48%Dutch study no overall survival benefit. (TME was standard)Key pointPreoperative radiation therapy led to a significant decrease in local reduction rate but no overall survival benefitQuestionHow do we further improve local control and overall survival?
11. 1997 Swedish rectal cancer trial.Randomized control trial. Neoadjuvant short course radiation therapy followed by surgery versus surgery alone.Significant decrease in local recurrence rate with neoadjuvant RT. 11% versus 27%.Significant increase in overall survival with neoadjuvant radiation therapy. 58% versus 48%.Caveat. Hospitals were not yet using TME as optimal surgery for rectal cancer. Thus, it is possible that neoadjuvant radiation therapy partially compensated for the suboptimal surgeries performed at that time. Note. Only study that had shown an improvement in overall survival with preoperative radiation therapy.2001. Dutch colorectal cancer trial.Neoadjuvant radiation therapy followed by surgery. Versus surgery alone.Surgery was standard TME protocol.Significant decrease in local recurrence rate with radiation therapy preoperatively compared to surgery alone.Local recurrence rate 2.4% versus 8.2%2-year overall survival rate was 82% in both arms. Note that TME was the standardized surgical procedure.
12. CHEMOTHERAPYRationaleTravels all over the body Potential to kill microscopic local as well as distant metastatic diseaseMakes radiation therapy work better High-dose chemotherapy depletes immune cells Standard dose chemotherapy impairs immune cells Low-dose chemotherapy selectively impairs certain immune cells T Reg and MDSC cells shield normal cells from cytotoxic T cells and NK cells preventing damage to normal cells But they also shield cancer cellsLow-dose chemotherapy selectively impairs T Reg and MDSC cells KEY POINTLow-dose chemotherapy weakens cancer cells, making them more susceptible to radiation treatment
13. ? ADD CHEMOTHERAPY TO RT (NEOADJUVANT CHEMO RT)Multiple strategies. German study 2004. EORTC study 2006. Neoadjuvant radiation therapy, TME, adjuvant chemotherapy Neoadjuvant radiation therapy, TME Neoadjuvant low dose concurrent chemotherapy + RT, TME, adjuvant chemotherapy TME, chemotherapy + concurrent RT, adjuvant therapyKEY POINT. Both studies showedNeoadjuvant low dose chemotherapy concurrent with RT was significantly better than all strategies Significant decrease in local recurrence rate. Decreased short-term and long-term toxicity Increased rate of sphincter preservation Increased rate of overall compliance with treatment No overall survival benefit6 13, 9 17
14. LANDMARK STUDY THAT SHAPED THE STANDARD OF CARE FOR RECTAL CANCER LARC. German colorectal study group.2004Preoperative chemotherapy + concurrent radiation therapy, surgery, followed by adjuvant chemotherapy versusSurgery, Postoperative chemotherapy + concurrent RT, followed by adjuvant chemotherapyAt 5 years the local recurrence rate in the preoperative CRT was 6% versus 13% P0.0065-year overall survival was the same 76% and 74%Acute toxicity grade 3/4 preoperative CRT 27% versus 40%. (P001)Long-term toxicity preop CRT 14% versus 24% in the postop group (P.01)The preoperative treatment consisted of 5040 cGy delivered in fractions of 180 cGy per day, five days per week, and fluorouracil, given in a 120-hour continuous intravenous infusion at a dose of 1000 mg per square meter of body-surface area per day during the first and fifth weeks of radiotherapy. Surgery was performed six weeks after the completion of chemoradiotherapy. One month after surgery, four five-day cycles of fluorouracil (500 mg per square meter per day) were given. Chemoradiotherapy was identical in the postoperative-treatment group, except for the delivery of a boost of 540 cGy. Study established that preoperative chemo RT versus postoperative chemo RT reduce local recurrence rates, decrease toxicity both acute and long-term, increased overall compliance, and increased sphincter preservation.Study was widely accepted and became that the standard of care for treatment of LARC.
15. Jean-François Bosset , EORTC Radiotherapy Group Trial 22921Preop RT vs Preop CRT+ Adjuvant chemo vs Preop RT+ adjuvant chemo vs preop CRT + Adjuvant chemoPreoperative chemotherapy TWO 5-day courses during Wk 1 and 5 of RT. Fluorouracil was given at a dose of 350 mg per m/2/day, and leucovorin at a dose of 20 mg mg/m2/day. Postoperative chemotherapy was delivered in 4 courses, every 3 weeks, with the same scheme and doses that were used preoperatively.Preop RT local recurrence rate 17%Preop chemo RT 9% (2 cycles of 5-FU/leucovorin preop)Preop RT plus postop chemo 9% (4 courses of postop chemo)Preop chemo RT plus postop chemo 8% (2 cycles chemo preop, 2 cycles chemo postop)Superior local control rates with chemo RT preop compared to preop RT alone.No overall survival benefit.
16. WHY NO OVERALL SURVIVAL BENEFIT WITH CHEMOSTAGE III COLON CANCER, ADJUVANT CHEMOTHERAPY=OVERALL SURVIVAL BENEFITAdjuvant chemotherapy = FULL dose, not low dose. After surgery.Compliance rate with adjuvant chemotherapy was very poor (43 to 55%)Significant delays in starting adjuvant chemotherapy due to postop complicationsPatients unable to get the recommended doses due to toxicityPatients unable to get recommended doses at recommended intervalsSignificant more toxicity getting adjuvant chemotherapy postopChemo regimens used then were quite different from what is the standard of care today
17. OPTMIZING TUMOR RESPONSE? Give ALL therapy before surgery (TNT)? Increase the INTERVAL between preop therapy and surgery? RT/concurrent chemo full dose chemo surgery ? full dose chemo RT/concurrent chemo surgery? Combination of above
18. TNT=RADIATION/CHEMO LOW DOSE+ FULL DOSE CHEMO, THEN SURGERYRationale for giving FULL DOSE chemotherapy before surgeryEarly treatment of micrometastatic diseaseDecrease in distant metastasesIncrease in survival rates as a result of decrease in distant metastasesLess toxicity. Easier to tolerate chemo preop = Better complianceAdminister all the treatments without significant delays or discontinuing treatmentAchieve better tumor regression locally in the rectum (pCR). With better pCR, ? increase the odds of organ preservation in selected patients.
19. 2 PIVOTAL TRIALS WITH TNT APPROACH TNT VS STANDARD OF CARE (CHEMO/RT, TME, ADJUVANT CHEMO) 2020 Arthur Affleck IV
20. RAPIDO AND PRODIGE 2020 TNT VS STANDARD OF CARE (CHEMO/RT,TME, ADJUVANT CHEMO)SIGNIFICANT IMPROVEMENT IN pCR RATES28% VS 14%, 28% VS 12%SIGNIFICANT DECREASE IN DISTANT METASTASES20% VS 27% RAPIDOSIGNIFICANT DECREASE IN DISEASE RELATED TREATMENT FAILURE24% VS 31% RAPIDOSIGNIFICANT IMPROVEMENT IN METASTASES FREE SURVIVAL80% VS 70% PRODIGESIGNIFICANT IMPROVEMENT IN DISEASE FREE SURVIVAL76% VS 69% PRODIGEOVERALL SURVIVAL SAME AT 3 YEARS89% VS 89% RAPIDO 91% VS 88% PRODIGE
21. RAPIDO (2020)Short course radiation therapy, followed by chemotherapy, (FOLFOX 4 /Cape ox for 18 weeks, followed by TME versus CRT, TME, adjuvant chemotherapy (Cape ox/FOLFOX) 24 weeks.Improved 3-year disease related treatment failure with TNT 24 versus 31% (significant)Increased PCR 28% versus 14%. SignificantDecreased distant metastases 20% versus 27% P significantOverall survival at 3 years was the same at 89%.Local recurrence rate is the same in both armsPRODIGE (2020)FOLFOX (6 cycles, 12 weeks), long course chemoradiation therapy, TME, Cape ox/FOLFOX x4 cycles (8 weeks) versus long course chemoradiation therapy, TME, Cape ox/FOLFOX x24 weeks (12 cycles)3-year disease-free survival 75% versus 68% (significant) and increased PCR 28% versus 12%3-year metastases free survival 79% versus 71% P significant. Overall survival of 91% versus 88%. P not significant.Local recurrence rate not reached.
22. ?OPTIMAL SEQUENCE OF TNTFACTNEOADJUVANT FULL DOSE CHEMOTHERAPY ADDED TO NEOADJUVANT RT = BETTER OUTCOMES AND BETTER ODDS OF ORGAN PRESERVATION (NO COLOSTOMY)LONGER INTERVAL FROM NEOADJUVANT THERAPY TO SURGERY= BETTER LOCAL TUMOR RESPONSE(pCR)SO WHICH SEQUENCE IS POTENTIALLY BETTER ?RT+LOW DOSE CHEMO FULL DOSE CHEMO TME ORFULL DOSE CHEMO RT+LOW DOSE CHEMO TME25 18
23. OPTIMAL SEQUENCE OF TNTRT+LOW DOSE CHEMO FULL DOSE CHEMO TME (consolidation) FULL DOSE CHEMO RT+LOW DOSE CHEMO TME (induction)CAO/ARO/AIO 12(2019) Consolidation arm Higher pathologic Complete Response (pCR) Less toxicity, increased compliance with all Rx Better odds of Organ PreservationDisease Free Survival at 4 years same between the 2 armsLocal recurrence rates same between the 2 arms 25 17 75 5 6
24. OPTIMAL SEQUENCE OF TNT/ OPRART+LOW DOSE CHEMO FULL DOSE CHEMO TME/WATCH & WAIT* (consolidation) FULL DOSE CHEMO RT+LOW DOSE CHEMO TME/WATCH & WAIT* (induction)OPRA TRIAL 2020At 3years NO COLOSTOMY/NO TMEInduction arm 47%Consolidation arm 60%Tumor regrowth -- less in consolidation armDisease Free Survival same in both arms compared to historical controls *WATCH AND WAIT APPROACH WITH NO TME, ONLY IF IN COMPLETE CLINICAL RESPONSE (cCR) or NEAR COMPLETE cCR27 40 75
25. THE TIMING OF RECTAL CANCER RESPONSE TO CRT CONSORTIUM TRIAL 2015Increase pCR 18% to 25% when average time from RT to surgery was increased to 6 to 11 weeksGERMAN 2019 CAO/AR/AIO 12.Phase 2 RCT of 2 TNT approachesInduction chemotherapy with FOLFOX followed by CRT, followed by TME. CRT was 5-FU oxaliplatinVersus CRT followed by chemotherapy and TME. CRT was the same with 5-FU approximately, chemo was FOLFOX.pCR 25% versus a 17%Lower toxicityBetter compliance with CRTPotentially better chances of organ preservationOPRA TRIAL TNT TME/WW 2020/2022CRT CHEMO TME/WW 5FU or CAP+RT, FOLFOX/CAPOX x 4 months orCHEMO/CRT TME/WW FOLFOX/CAPOX x 4 months, 5FU or CAP+RTOS not reached. DFS 76% @ 3 yrs, same as historical controlsConsolidation arm, 60% colostomy free vs 47% in induction armDistant met rate 20% @ 3 years, same as RAPIDOLocal regrowth 20 vs 40 consolidation vs induction
26. WATCH AND WAIT APPROACH ONLY for clinical Complete response/near cCRSurveillance FindingsDRE smooth, normal mucosaEndoscopy flat white scar, telangiectasia, absence of both ulcer and nodularityMRI scar not thicker than the rectal wall, dark T2 signal and no visible lymph nodesSTRICT SurveillanceDRE, endoscopy, CEA every 4 months x 2 years, every 6 months x3 yearsRectal MRI every 6 months for 2 years, then annually. CT chest abdomen pelvis annually.NOTE:Local recurrence about 25%Local recurrence occurred within the first 2 yearsSurgical salvage successful in over 90% of these patients5-year overall survival 85%5-year disease specific survival 94%Potential increased chance of distant metastases in those with local regrowth 18% versus 5% in those with no regrowthIMPORTANT TO HAVE THE DISCUSSION WITH PATIENTS
27. ? AVOID CHEMO/RADIATION/SURGERYMSI-High/MMR-deficient rectal cancerStage II/III 5 to 10% will be MMR-dImmunotherapy (dostarlimab-gxly) 2022Majority had bulky tumors, 94% node+100% clinical COMPLETE RESPONSE @ 6 MONTHSLonger follow up neededImmunotherapy will potentially benefit only about 5 to 10% of all rectal cancer patientsCercek et al, JCO 2020,38,TPS4123
28. WHAT WE KNOW TNT versus CRT TME ADJUVANT CHEMOTNT SHOULD BE STANDARD FOR STAGE II AND III RECTAL CANCERPREFERRED OPTION IN NCCNPREFERRED SEQUENCE:RT+ LOW DOSE CHEMO, THEN FULL DOSE CHEMO = INCREASED pCR RATES & cCR RATES. INCREASED ORGAN PRESERVATION RATES BETTER QUALITY OF LIFELOS
29. WHAT WE KNOW TNT versus CRT TME ADJUVANT CHEMO:INCREASED DISEASE-FREE SURVIVALDECREASED LOCAL RECURRENCE RATESDECREASED DISTANT METASTASESDECREASED TREATMENT RELATED FAILUREDECREASED TOXICITY
30. CASE83-year-old male diagnosed with stage III rectal cancer. Which of the following treatments would be potentially appropriate?SurgeryRadiation therapyChemotherapyImmunotherapy Alone
31. CASE83-year-old male diagnosed with a stage III rectal cancer. Which of the following treatments would be potentially appropriate?Surgery Yes Possibly No in some patientsRadiation therapy Yes Possibly No in some patientsChemotherapy Yes Possibly No in some patientsImmunotherapy Alone YES !!
32. SO1. The Rx of locally advanced rectal cancer has evolved dramatically over the last 20 years.2. Multidisciplinary approach3. One size fits all no longer appropriate. Rx needs to be individualized. 4. A good proportion of patients may be spared surgery.5. Very small proportion of patients may be spared surgery, chemotherapy and radiation and be treated with immunotherapy alone.