
1 Pelvic organ prolapse POP 2 Pelvic organ prolapse POP Definition Decent of one or more of the pelvic organs uterus urinary bladder urethra rectum and loops of bowel downwards into the vagina ID: 919358
Download Presentation The PPT/PDF document "Urogynecology Done by: Thaer Omar Alqat..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
Urogynecology
Done by: Thaer Omar Alqatish
1
Slide2Pelvic organ prolapse (POP)
2
Slide3Pelvic organ prolapse (POP)
Definition Decent of one or more of the pelvic organs (uterus, urinary bladder, urethra, rectum , and loops of bowel), downwards into the vagina.Epidemiology
Common problem in women(12-30% of women) Increase significantly by both age and
multiparity
(or large birth)
.
Surgery
, 5-7% develop post-hysterectomy vault prolapseIncrease intra-abdominal pressure (obesity, straining, chronic cough, chronic constipation,….)
3
Slide4Anatomy
** Structures that supports the pelvic organs: a. Transverse cervical ligament b. Uterosacral ligament c. Pubocervical
ligamentd. Pelvic floor muscles: The levator
ani
muscles (
Ischio-coccygeus
muscle,
Ilio-coccygeus muscle, Pubo-coccygeus muscle)
4
Slide55
Slide6Types of POP
1) Anterior vaginal wall prolapse (anterior compartment) - Urethrocele, Cystocele
, cysto-urethrocele. 2) Posterior vaginal wall prolapse (posterior compartment) -
Rectocele
,
Enterocele
.
3) Apical vaginal prolapse (central compartment) - Utero-vaginal prolapse, Vault prolapse
6
Slide77
Slide8Presentation & dx
They all present with > vaginal fullness & back pain Presentation specific to the type: Cystocele (urine incontinence), rectocele (constipation, fecal incontinence)Dx > clinically (speculum examination)
8
Slide9Cystocele
9
Slide10Rectocele
10
Slide11Uterine prolapse
11
Slide12POP grading system
12
Slide13Baden Walker Grading of POP
13
Slide14Congenital POP
Congenital weakness of the pelvic supports associated with:
1) Short vagina 2) Spina
bifida
3) Deep
uterovaginal
, and uterosacral pouches
14
Slide15Treatment of POP
1. Conservative Pelvic floor physiotherapy (Kegal exercises)Vaginal pessary
2. Surgical:basically, remove or repair the uterus (Hysterectomy or hysteropexy
)
Rectocele or cystocele repair (
colporrhaphy
, anterior & posterior repair)
15
Slide16Pessary
A pessary is a prosthetic device that can be inserted into the vagina to support its internal structure (either lifts the bladder or apply compression to the urethra preventing leakage).
16
Slide17Indications for surgical tx
1. Failed conservative 2. Severe degree 3. Pt. doesn’t desire to preserve fertility
17
Slide18Anterior repair
18
Slide19Posterior repair Perineal reconstruction
19
Slide20Hysterectomy or hysteropexy
To preserve fertility > go for hysteropexy.If no worries about fertility > you can go for Hysterectomy (also
eliminates risk of cervical / uterine pathology)
20
Slide21Complications of surgical tx:
1. General complications Anesthetic problemsBleeding: Serious requiring transfusion ( < 1%)
Post operative infectionUTI : 6% if a catheter has been used2. Specific complications
Injury to bladder, urethra, ureters, rectum
Postoperative stress urinary Incontinence
21
Slide22Urinary incontinence
Definition is the inability to hold urine, producing involuntary urinary leakage > resulting in hygiene & social concerns.
EpidemiologyThe prevalence increases with age
,
with approximately
5 % of women between 15 and 44 years of age being affected, rising to 10 % of those aged between 45 and 64 years, and approximately 20 % of those older than 65 years
.
SmokingPregnancy & childbirth
Increase
intrabdominal
pressure > chronic cough, constipation, occupational lifting.
Menopause
22
Slide23Physiology of continence
Mechanical
Neural
23
Slide24Classification of Incontinence
Urodynamic stress incontinence (USI)Motor Urge (Hypertonic) IncontinenceOverflow (Hypotonic) IncontinenceSensory
Irritative IncontinenceFistula
24
Slide25Dissecting incontinence case
1- History > is there an urge to void ? is there nocturnal symptoms?
2- pay attention to the PE, UA, cystometry
25
Slide2626
Slide27The following are parameters of normal bladder function:
Residual urine of <50 mL.First desire to void between 150 and 200mL.
Capacity between 400 and 600 mL.
Detrusor pressure rise of <15 cmH2O during filing and
standing.
Absence of systolic detrusor contractions.
No
leakage on coughing.
27
Slide28Urodynamic stress incontinence
is defined as the involuntary leakage of urine during increased abdominal pressure in the absence of a detrusor contraction (the pressure rise forms outside the bladder
).This is the most common incontinence in young women
.
Causes
: loss of pelvic support (birth, menopause, congenital) , increasing
intrabdominal
pressure (chronic cough, constipation, etc..)28
Slide29History
No urge > loss of urine occurs in small spurts simultaneously with coughing or sneezing. No nocturnal symptoms > it
does not take place when the patient is sleeping. Examination
Pelvic
examination may reveal a cystocele
.
Neurologic
examination is normal. Q tip test??Investigative studies
.
Urinalysis
and culture are normal.
Cystometric
studies are normal with no involuntary
detrusor contractions
seen.
29
Slide3030
Slide31Management
Conservative > Kegel exercises & pessariesSurgical tx >
(Burch procedure or Marshall
Marchetti-Kranz
(MMK)
procedure) {basically
elavate
& attach the urethral sphincter to the symphysis pubis} > A minimally invasive surgical procedure is the tension-free vaginal tape procedure in which a mesh tape is placed
transcutaneously
around and under the mid
urethra.
31
Slide3232
Slide33Motor Urge (Hypertonic) Incontinence
This is the most common incontinence in older womenEtiology: involuntary rises in bladder pressure occur from idiopathic detrusor contractions that cannot be voluntarily suppressed.
33
Slide34History
Loss of urine occurs in large amounts often without warning. This can take place both day and night. The most common symptom is urgency.Examination Pelvic examination shows normal anatomy. Neurologic examination is normal.
Investigative studies Urinalysis
and culture
are normal
.
Cystometric
studies show normal residual volume, but involuntary detrusor contractions are present even with small volumes of urine in the bladder.
34
Slide3535
Slide36Management
Anticholinergic medications (e.g., oxybutynin [Ditropan]) Side effects??; nonsteroidal anti-inflammatory drugs (NSAIDs) to inhibit detrusor contractions; tricyclic antidepressants; calcium-channel
blockers.Second-line treatmentEndoscopic injection of botulinum toxin at different points in the bladder wall
Sacral nerve stimulation
36
Slide37Overflow (Hypotonic) Incontinence
It’s leakage secondary to over-distended bladder, which becomes higher than urethral pressure. There is no or poor bladder contractionEtiology: Denervated
bladder (e.g., diabetic neuropathy, multiple sclerosis)Medication
like anti-cholinergic or
alpha agonist
Urethral
obstruction
37
Slide38History
Loss of urine occurs intermittently in small amounts. This cantake place both day and night. The patient may complain of pelvic fullness. Examination
Pelvic examination may show normal anatomy; however, the neurologic examination will show decreased pudendal nerve sensation.
Investigative studies
Urinalysis
and culture are usually normal, but may show
an infection. Cystometric studies show markedly increased residual volume, but involuntary detrusor contractions do not occur.
38
Slide3939
Slide40Management
Treatment of underlying conditionintermittent self-catheterizationCholinergic medications to stimulate bladder contractions
40
Slide41Sensory Irritative Incontinence
Etiology: Detrusor contractions stimulated by irritation from any
of the following bladder conditions: infection, stone, tumor, or a foreign body.
41
Slide42History
Loss of urine occurs with urgency, frequency, and dysuria. This can take place day or night.Examination Suprapubic
tenderness may be elicited, but otherwise the pelvic examinationis unremarkable. Investigative
studies
A urinalysis will show the following abnormalities: bacteria and white blood cells (suggest an infection) or red blood cells (suggest a stone, foreign body, or tumor
).
A urine culture is positive if an infection is present. Cystometric
studies (which are usually unnecessary) would reveal normal residual volume with involuntary detrusor contractions present.
42
Slide43Management
Treat the underlying problemInfections are treated with antibiotics. Cytoscopy is used to diagnose and remove stones, foreign bodies, and tumors.
43
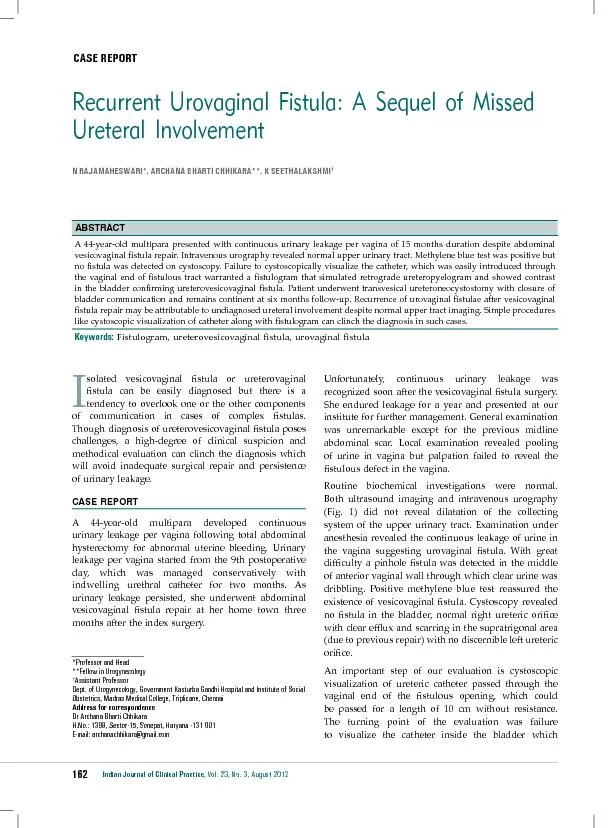
Slide44Fistula incontinence
Caused by inflammation, radiation, surgery, Ca, IBD. Can be uretrovaginal, vesicovaginal
and urethrovaginal.History
The
patient usually has a history of radical pelvic surgery or pelvic
radiation therapy
. Loss of urine occurs continually in small amounts. This can take place both day and night
.
Examination
Pelvic
examination may show normal anatomy and normal neurologic
findings
Investigative studies
Urinalysis
and culture are normal.
Tampon test ??
Management
: surgical (
fistulotomy
or
fistulectomey
)
44
Slide45Tampon test
45
Slide46Congenital causes
EpispidiasHypospadiasBladder exstrophyEctopic ureter
46
Slide4747
Slide4848