
Authored by Prof Michael C Herbst D Litt et Phil Health Studies D N Ed M Art et Scien B A Cur Dip Occupational Health Approved by Ms Elize Joubert C hief E xecutive O fficer BA Social Work ID: 951727
Download Pdf The PPT/PDF document "Researched and" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






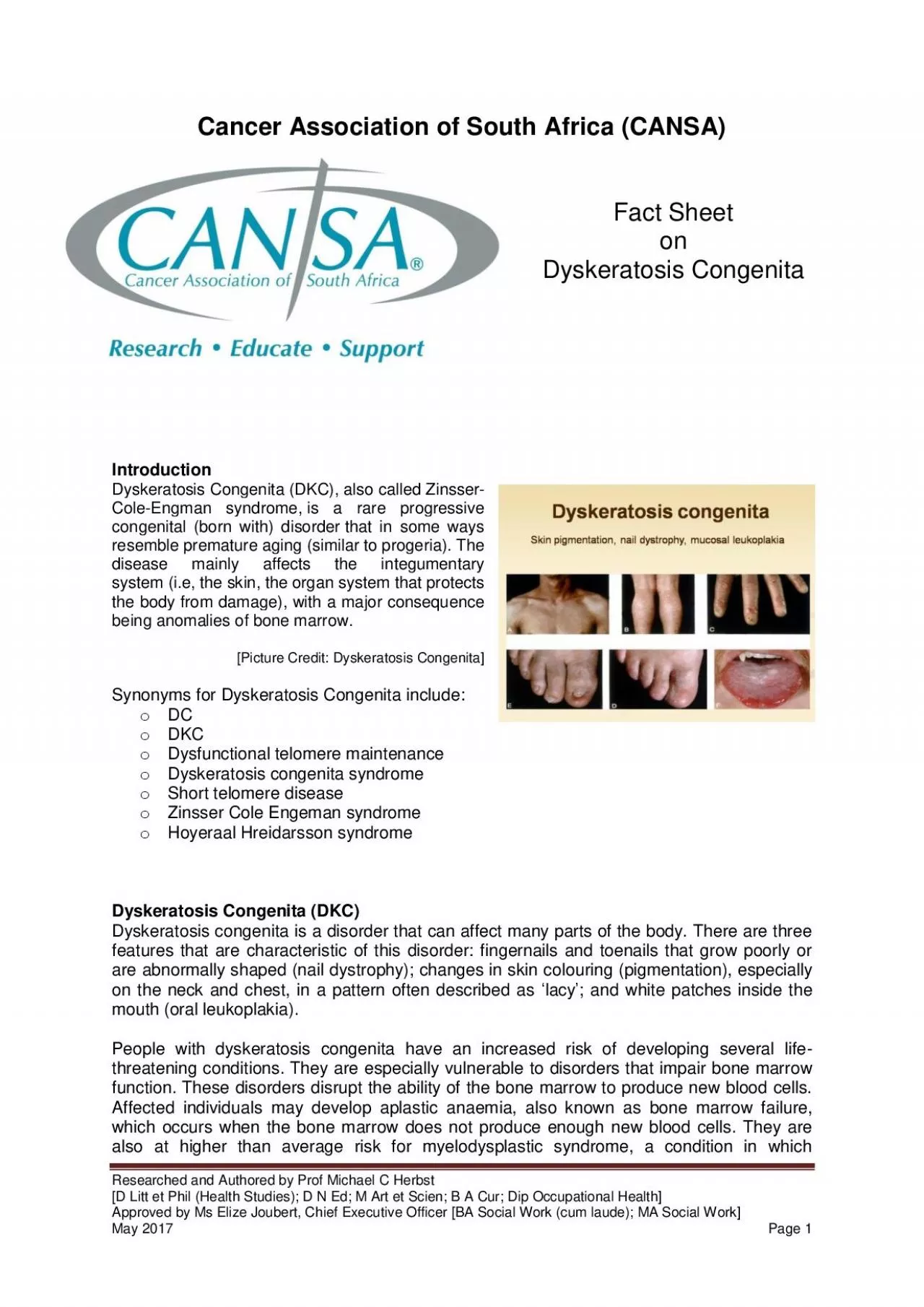
Researched and Authored by Prof Michael C Herbst [D Litt et Phil (Health Studies); D N Ed; M Art et Scien; B A Cur; Dip Occupational Health] Approved by Ms Elize Joubert, C hief E xecutive O fficer [BA Social Work (cum laude); MA Social Work] May 201 7 Page Cancer Association of South Africa (CANSA) Fact Sheet o n Dyskeratosis Congenita Introduction ongenita (DKC), also called Zinsser - Cole - Engman syndrome , is a rare progressive congenital (born with) disorder that in some ways resemble premature aging (similar to progeria). The system (i.e, the skin, the organ system that protects the body from damage), with a major consequence being anomalies of bone marrow. [Picture Credit: Dyskeratosi s Congenita] Synonyms for Dyskeratosis Congenita include: o o DKC o Dysfunctional telomere maintenance o Dyskeratosis congenita syndrome o Short telomere disease o Zinsser Cole Engeman syndrome o Hoyeraal Hreidarsson syndrome Dyskeratosis Congenita (DKC) Dyskeratosis congenita is a disorder that can affect many parts of the body. There are three are abnormally shaped (nail dystrophy); changes in skin colo u ring ( pigmentation), especially on the neck and chest, in a pattern often described as ‘ lacy ’ ; and white patches inside the mouth (oral leukoplakia). People with dyskeratosis congenita have an increased risk of developing several life - threatening conditions. Th function. These disorders disrupt the ability of the bone marrow to produce new blood cells. Affected individuals may develop aplastic an a emia, also known as bone marrow failure, which occur s when the bone marrow does not produce enough new blood cells. They are also at higher than average risk for myelodysplastic syndrome, a condition in which Researched and Authored by Prof Michael C Herbst [D Litt et Phil (Health Studies); D N Ed; M Art et Scien; B A Cur; Dip Occupational Health] Approved by Ms Elize Joubert, C hief E xecutive O fficer [BA Social Work (cum laude); MA Social Work] May 201 7 Page 2 immature blood cells fail to develop normally; this condition may progress to a form of blood cance r called leuk a emia. People with dyskeratosis congenita are also at increased risk of developing leuk a emia even if they never develop myelodysplastic syndrome. (Please refer to the Fact Sheet on Myelodysplastic Syndrome – available on www.cansa.org.za ). In addition, they have a higher than average risk of developing other cancers, especially c
ancers of the head, neck, anus, or genitals. People with dyskeratosis congenita may also develop pulmonary fibrosis, a condition that causes scar tissue (fibrosis) to build up in the lungs, decreasing the transport of oxygen into the bloodstream. Additional signs and symptoms that occur in some people with dyskeratosis congenita include eye abnormalities such as narrow tear ducts that may become blocked, preventing dr ainage of tears and leading to eyelid irritation; dental problems; hair loss or prematurely grey hair; low bone mineral density (osteoporosis); degeneration (avascular necrosis) of the hip and shoulder joints; or liver disease. Some affected males may have narrowing (stenosis) of the urethra, which is the tube that carries urine out of the body from the bladder. Urethral stenosis may lead to difficult or painful urination and urinary tract infections. The severity of dyskeratosis congenita varies widely am ong affected individuals. The least severely affected individuals have only a few mild physical features of the disorder and normal bone marrow function. More severely affected individuals have many of the characteristic physical features and experience bo ne marrow failure, cancer, or pulmonary fibrosis by early adulthood. [Picture Credit: Dyskeratosis Congenita 2] While most people with dyskeratosis congenita have normal intelligence and development of motor skills such as standing and walking, developmental delay may occur in some severely affected individuals. In one severe form of the disorder called Hoyeraal Hreidaarsson syndrome, affected individuals have an unusually small and underdeveloped cerebellum, which is the part of the brain that coordinates movement. Another severe variant called Revesz syndrome involves abnormalities in the light - sensitive tissue at the back of the eye (retina) in addition to t he other symptoms of dyskeratosis congenita. (Genetics Home Refere4nce). The disease is characterised by multisystem failure, affecting essentially tissues with a high proliferation rate: skin, mucous membranes and bone marrow. o Short stature (16%) o Cutaneous (skin) signs: Hyperpigmentation, telangiectasia, atrophy (poikilodermia) Dystro p hic nails and palmoplantar keratoderma, hyperhidrosis Mucosal leukoplakia Dental caries or loss (18%) Blepharitis, conjunctivitis, epiphora (36%) Sparse eyebrows / ey elashes Researched and Authored by Prof Michael C Herbst [D Litt et Phil (Health Studies); D N Ed; M
Art et Scien; B A Cur; Dip Occupational Health] Approved by Ms Elize Joubert, C hief E xecutive O fficer [BA Social Work (cum laude); MA Social Work] May 201 7 Page 3 Alopecia (16%) Urethral stricture, phimosis (7%) o Bone marrow failure, peripheral pancytopenia (93%) o Other si g ns: Oesophageal stricture (14%) Pulmonary fibrosis (19%) Liver cirrhosis (5%) Hypogonadism (8%) Abnormal bvone trabeculation, osteoporosis (4%) o Immune abnormalities: reduced or increased immunoglobulin level, T - and/or B - lymphocyte deficiency o Mild mental retardation, learning difficulties (21%) o About 90% of affected individuals are males ( Atlas of Genetics and Cytogenetics in Oncology and Hae matology ) Occurrence of Leukaemia and Cancer Individuals with D yskeratosis C ongenita also have a predisposition to develop leukaemia and cancer (malignancy) especially squamous cell carcinoma of the head and neck, and especially at the site of leukoplakia. If cancer occurs, it usually does not develop until the age of about 30. Thus, leukaemia and cancer are more common in individuals who hav e a moderate or milder form of D yskeratosis C ongenita. Individuals who underwent a stem cell or bone marr ow transplant for the treatment of their bone marrow failure are also at risk of developing cancer later in life. In rare cases leukaemia or cancer may be the first manifestation of disease (NORD). Dyskeratosis Congenita (D K C) in Children Dyskeratosis C ongenita (D K C) is caused by a change (mutation) in genes. Sometimes, this change happens in a child with D K C without being passed on by their parents. Most often, though, the genes that are not working correctly are passed to children by their parents. Som e parents of children with D K C may have the disease but might not have obvious signs of it. Babies are born with D yskeratosis C ongenita , although symptoms of the disease may not show up for years, and sometimes even for decades. Some babies are diagnosed with D yskeratosis C ongenita soon after they are born. Other people do not get a diagnosis until they are adults. Most often, doctors find the diso rder when a person is between 10 and 30 years old. (Seattle Children’s Hospital Research Foundation). Incidence of Dyskeratosis Congenita (D K C) in South Africa Because Dyskeratotis Congenita is primarily a non - cancerous condition, the National Cancer Re gistry (20 1 2 ) does not provide any information on th
is condition. D K C is a precursor to blood problems, including leukaemia. The South African National Cancer Registry (20 1 2 ) does not provide information regarding the different types of leukaemia – they are all grouped together and listed as ‘Leukaemia’. Researched and Authored by Prof Michael C Herbst [D Litt et Phil (Health Studies); D N Ed; M Art et Scien; B A Cur; Dip Occupational Health] Approved by Ms Elize Joubert, C hief E xecutive O fficer [BA Social Work (cum laude); MA Social Work] May 201 7 Page 4 In providing the incidence figures of leukaemia in South Africa, The National Cancer Registry does not make provision for the reporting of the different types of leukaemia – it also does not differentiat e between acute and chronic leukaemia - neither does it provide for different statistics for cases of adult and childhood leukaemia. According to th e National Cancer Registry (2012 ) the following number of L eukaemia cases w as histologically diagnosed in South Africa during 20 12 : Group - Males 20 12 Actual No of Cases Estimated Lifetime Risk Percentage of All Cancers All males 380 1:502 1,03% Asian males 11 1:666 1,34% Black males 201 1:762 1,73% Coloured males 42 1:452 0,97% White males 126 1:232 0,63% Group - Females 20 12 Actual No of Cases Estimated Lifetime Risk Percentage of All Cancers All females 285 1:955 0,76% Asian females 5 1:1 777 0,47% Black females 160 1:1 409 0,97% Coloured females 49 1:440 1,17% White females 72 1:480 0,45% The frequency of histologically diagnosed cases of L eukaemia in South Africa for 20 12 w as as follows (National Cancer Registry, 20 12 ): Group - Males 2012 0 – 19 Years 20 – 29 Years 30 – 39 Years 40 – 49 Years 50 – 59 Years 60 – 69 Years 70 – 79 Years 80+ Years All males 88 29 38 42 50 54 54 20 Asian males 3 1 0 0 1 2 2 2 Black males 67 21 25 20 20 23 13 3 Coloured males 6 2 5 1 8 6 8 4 White males 12 5 6 18 18 23 30 11 Group - Females 2012 0 – 19 Years 20 – 29 Years 30 – 39 Years 40 – 49 Years 50 – 59 Years 60 – 69 Years 70 – 79 Years 80+ Years All females 63 19 24 34 42 37 31 20 Asian females 0 1 1 2 1 0 0 0 Black females 40 18
27 16 22 11 12 6 Coloured females 10 4 3 3 5 13 5 5 White females 12 3 1 6 14 12 14 9 N.B. In the event that the totals in any of the above tables do not tally, this may be the result of uncertainties as to the age, race or sex of the individual. The totals for ‘all males’ and ‘all females’, however, always reflect the correct totals. Causes of Dyskeratosis Congenita (D K C) To date, there are 10 known genes that identify with D K C - DCK1 , TERC , TERT , NOP10 , NHP2 , TINF2 , USB1 , TCAB1 , CTC1 , and RTEL1 ). D K C is genetically heterogeneous, with X - linked recessive (Mendelian Inheritance in Man [MIM] 305000), autosomal dominant (MIM 127550), and autosomal recessive (MIM 224230) subtypes. D K C is related to telomerase dysfunction; all genes associated with this syndrome (i.e., DKC1 , TERT, TERC, NOP10 ) encode proteins in the telomerase complex responsible Researched and Authored by Prof Michael C Herbst [D Litt et Phil (Health Studies); D N Ed; M Art et Scien; B A Cur; Dip Occupational Health] Approved by Ms Elize Joubert, C hief E xecutive O fficer [BA Social Work (cum laude); MA Social Work] May 201 7 Page 5 for maintaining telomeres at the ends of chromosomes regarding shortening length, protection, and replication. In the X - linked recessive form, the gene defect lies in the DKC1 gene (located at Xq28), which encodes for the protein dyskerin. Dyskerin is c omposed of 514 amino acids and has a role in ribosomal RNA processing and telomere maintenance. Modification of dyskerin by SUMOylation has been shown to stabilize the protein. In addition, a mutation in the DKC1 gene is also found on exon 15, revealing a duplication, which adds a lysine residue on a polylysine tract on the C - terminus. All in all, there have been over 50 mutations found in DKC1 . In the autosomal dominant form, mutations in the RNA component of telomerase ( TERC ) or telomerase reverse trans criptase ( TERT ) are responsible for disease phenotype. Defects in the NOP10 gene were found in association with autosomal recessive D K C. NOP10 encodes small nucleolar ribonucleoproteins (snoRNP) associated with the telomerase complex. In persons with aut osomal dominant D K C and in terc - / - knockout mice, genetic anticipation (i.e., increasing severity and/or earlier disease presentation with each successive generation) has been reported. A heterozygous mutation was found on the conserved telomere main
tena nce component 1 gene ( CTC1 ). This implication is also associated with a pleiotropic syndrome, Coats plus. Homozygous autosomal recessive mutations in RTEL1 lead to similar phenotypes that parallel with Hoyeraal - Hreidarsson (HH) syndrome. It is associated with short, heterogeneous telomeres. In the presence of functional DNA replication, RTEL1 mutations produce a large amount of extrachromosomal T - circles. Enzymes remove the T - circles and therefore shorten the telomere. RTEL1 has a role in managing DNA damage by increasing sensitivity; therefore, mutations on this gene cause both telomeric and nontelomeric causes of D K C. Patients with D K C have reduced telomerase activity and abnormally short tracts of telomeric DNA compared with normal controls. Telomeres are repeat structures found at the ends of chromosomes that function to stabilize chromosomes. With each round of cell division, the length of telomeres is shortened and the enzyme telomerase compensates by maintaining telom ere length in germline and stem cells. Because telomeres function to maintain chromosomal stability, telomerase has a critical role in preventing cellular senescence and cancer progression. Rapidly proliferating tissues with the greatest need for telomere maintenance (e.g, bone marrow) are at greatest risk for failure. DKC1 has been found to be a direct target of the c - myc oncogene, strengthening the connection between D K C and malignancy. Analysis of 270 families in the D K C registry found that mutations in dyskerin ( DKC1 ), TERT , and TERC only account for 64% of patients, with an additional 1% due to NOP10 , suggesting that other genes associated with this syndrome are, as yet, unidentified. In addition to the mutations that directly a ffect telomere length, r ecent studies also indicate that a D K C diagnosis should not be based solely on the length of the telomere, but also the fact that there are defects in telomere replication and protection. In addition, revertant mosaicism has been a new recurrent event in D K C. (Medscape). Researched and Authored by Prof Michael C Herbst [D Litt et Phil (Health Studies); D N Ed; M Art et Scien; B A Cur; Dip Occupational Health] Approved by Ms Elize Joubert, C hief E xecutive O fficer [BA Social Work (cum laude); MA Social Work] May 201 7 Page 6 Prognosis (Outcome) The major part of patients die before 20 years, mainly from infectious complications of immune deficiency. o 90% of patients have haematological abnormalit
ies when 30 year - old, and bone marrow failure is the main cause of early morbidity in 71% of cases. It can evolve toward aplastic anaemia or myelodysplasia. o The mucosal leukoplakia can transform into spinocellular carcinoma. o Other carcinomas can develop during the third decade of life: lung, colon, laryn x , oesoph agus, pancreas, Hodgkin’s disease. ( Atlas of Genetics and Cytogenetics in Oncology and Haematology) Medical Disclaimer This Fact Sheet is intended to provide general information only and, as such, should not be considered as a substitute for advice, me dically or otherwise, covering any specific situation. Users should seek appropriate advice before taking or refraining from taking any action in reliance on any information contained in this Fact Sheet. So far as permissible by law, the Cancer Association of South Africa (CANSA) does not accept any liability to any person (or his/her dependants/estate/heirs) relating to the use of any information contained in this Fact Sheet. Whilst CANSA has taken every precaution in compiling this Fact Sheet, neither it, nor any contributor(s) to this Fact Sheet can be held responsible for any action (or the lack thereof) taken by any person or organisation wherever they shall be based, as a result, direct or otherwise, of information contained in, or accessed through, this Fact Sheet. Researched and Authored by Prof Michael C Herbst [D Litt et Phil (Health Studies); D N Ed; M Art et Scien; B A Cur; Dip Occupational Health] Approved by Ms Elize Joubert, C hief E xecutive O fficer [BA Social Work (cum laude); MA Social Work] May 201 7 Page 7 Sources and References Atlas of Genetics and Cytogenetics in Oncology and Haematology http://atlasgeneticsoncology.org/Kprones/DyskeratosID10034.html Dyskeratosis Congenita http://www.lookfordiagnosis.com/mesh_info.php?term=dyskeratosis+congenita&lang=1 Dyskeratosis Congenita 2 http://www.gopixpic.com/480/dyskeratosis - congenita/http:%7C%7Cwww*huidziekten*nl%7Cafbeeldingen%7Cdyskeratosis - congenita - 1*jpg/ Genetics Home Reference http://ghr.nlm.nih.gov/condition/dyskeratosis - congenita Medscape http://emedicine.medscape.com/article/1110516 - overview#a0104 NORD http://www.rarediseases.org/rare - disease - information/rare - diseases/byID/896/viewFullReport Seattle Children’s Ho spital Research Foundation http://www.seattlechildrens.org/medical - conditions/heart - blood - conditions/dyskeratosis - cong