
Hypothalamus releases TRH Act on the pituitary gland to release TSH TSH causes the thyroid gland to release the thyroid hormones T 3 and T 4 TRH and TSH concentrations are inversely related to T ID: 909008
Download Presentation The PPT/PDF document "Thyroid and pregnancy Control of Thyroid..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
Thyroid and pregnancy
Slide2Control of Thyroid Function
Hypothalamus releases TRH
Act on the pituitary gland to release TSH
TSH causes the thyroid gland to release the thyroid hormones (T
3 and T4)TRH and TSH concentrations are inversely related to T3 and T4 concentrations. 99% circulating T3 and T4 is bound to TBG. 1%
free form Biologically Active
Slide3Physiologic Changes in Pregnancy
Pregnancy is a state of relative iodine deficiency, because:
- Active transport to fetoplacental unit
- Increase iodine excretion in urine, 2 fold (increased GFT & decreased renal tubular reabsorption) - Thyroid gland increases its uptake from the blood
Slide4TBG
- Increase (hepatic synthesis is increased)
TT4 & TT3
- Increase to compensate for this rise
FT4 & FT3 (crosses the placenta in the 1st half of pregnancy) - Decrease. FT4 are altered less by pregnancy, but do fall little in the 2nd & 3rd trimesters. TSH (does not cross placenta) - decreases in 1st trimester, between 8 to 14 wks HCG, HCG has thyrotropin-like activity - Increase in 2nd & 3rd trimester (Increased TBG)
Slide5Changes of Hormones in Pregnancy
Slide6Thyroid hormones in pregnancy
Maternal
Thyroid volume increases by 10–20% with increased vascularity and a rise in thyroglobulin during pregnancy.
Hepatic synthesis of thyroid-binding globulin (TBG) is increased with increase in total T4 and T3 concentrations
Levels of free T4 and free T3 may rise in the first trimester, due to a hCG thyrotropic effect, but then remain in the normal rangeTSH is usually within normal limits in pregnancy but can be suppressed particularly in the first trimester because there is a negative correlation that exists between TSH and hCG levels in the first half of pregnancyTSH receptor antibodies may cross the placenta when present in high concentrations but the titre decreases with the progression of pregnancy.
Slide7Fetal
TRH & TSH synthesis by 8–10 weeks
Thyroid hormone synthesis by 10–12 weeks
TSH, TBG, free T4 and T3 increase throughout gestation
Maternal TSH does not cross the placentaMaternal T4 and T3 does cross the placenta in small quantities for early fetal growth.
Slide8Hyperthyroidism
Causes of maternal hyperthyroidism:
Graves disease (90% of cases)
toxic noduletoxic multinodular goitre
hydatiform molehyperemesis gravidarum.
Slide9Maternal & fetal outcomes are worse in cases of uncontrolled hyperthyroidism, with higher rates of:
pre-eclampsia
thyroid storm and
thyrotoxic
heart failurefetal growth restrictionprematuritystillbirthsfetal or neonatal thyrotoxicosis neonatal hypothyroidism
Slide10Treatment
Medications
:
carbimazole (CBZ), methiamazole
(MMI) or propylthiouracil (PTU), cross the placenta, but PTU less so than CBZ and MMI.Surgery is rarely performed in pregnancy, possibly if drug resistance or serious side effects with antithyroid drugs, e.g. agranulocytosis. Radioactive iodine treatment is contraindicated during pregnancy and should be avoided for at least 6 months after treatment.
Slide11Hypothyroidism
Slide12Clinical / Subclinical Hypothyroidism
Clinical
Hypothyroidism
Subclinical
HypothyroidismTSHHigh (>10) High (>3 - <10) Free T4 LowNormal Free T3 Normal or lowNormal Serum TSH level > 3.0 mIU/l Subclinical hypothyroidism elevated TSH with normal FT4, FT3.
Slide13Epidermiology
Overt hypothyroidism complicates up to 3 of 1,000 pregnancies
Subclinical hypothyroidism is estimated to be 2-5 % (
Canaris GH, 2000)
Slide14Symptoms of Hypothyroidism
Slowing of metabolic processes:
Lethargy/fatigue weight gain cognitive dysfunction
cold intolerance constipation bradycardia
delayed relaxation of tendon reflexesslow movement and slow speechDeposition of matrix substances:Dry skin hoarseness edemapuffy face and eyebrow loss peri-orbital edemaenlargement of the tongueOthersDecreased hearing myalgia and paresthesia depressionmenorrhagia arthralgia pubertal delaygalactorrhea
Slide15Overlapping Complaints
Symptoms
Hypothyroidism
Pregnancy
FatigueConstipationHair LossDry SkinBrittle NailWeight GainFluid RetentionBradycardiaCarpel Tunnel Syndrome
Slide16Subclinical Hypothyroidism
Elevated TSH (
> 3.0
mIU/l)
with normal FT4, FT3.31 % with anti-TPO antibodyMore common on women with autoimmune diseases50 % hypothyroidism in 8 yearsMay cause childhood IQ decreaseIncrease in preterm 4% vs 2.5% in euthyroid mother (Casey BM, 2007)
Slide17Types of Hypothyroidism
Primary hypothyroidism
Secondary/tertiary hypothyroidism
IatrogenicEnvironmental
Slide18Primary Hypothyroidism
Developed Countries
Hashimoto’s thyroiditis – Chronic thyroiditis
prone to develop postpartum thyroiditis
WorldwideIodine deficiencyOther Causes:Subacute thyroiditisThyroidectomy, radioactive iodine treatment
Slide19Hashimoto’s Thyroiditis
An inflammatory disorder of thyroid gland
More common on those with other autoimmune diseases
Almost 100% associated with anti-TPO antibody. (Fitzpatrick & Russell)
May cause transient hyperthyroidismPE: Goiter, rubbery consistency, moderate in size, mostly bilateral, painless.
Slide20Hashimoto’s Thyroiditis
T cells recognize the patient’s own thyroid antigens as foreign
cytotoxic to thyroid epithelial cells
stimulate B cells to make anti-thyroid antibodies, anti-peroxidase antibody, anti-thyroglobulin antibody, and anti-TSH-receptor antibody block the action of TSH, leading to hypothyroidism!!
Slide21Hashimoto’s Thyroiditis
Lymphoid infiltrate, often with germinal centers
Slide22Iodine Deficiency
Affect 38% of worldwide population (Pearce EN, 2008)
Sources: Iodized salt and seafood. Others: cow milk, egg, beans…
Perinatal
mortalityCongenital cretinism (growth failure, mental retardation, other neuropsychological deficits) ACOG
Slide23Subacute Thyroiditis
Subacute granulomatous thyroiditis
- Painful - Fever, myalgia
- Viral infection
Subacute lymphocytic thyroiditis - includes postpartum thyroiditis (Prevalent: 5% ) - PainlessSymptomatic Tx for initial hyperthyroidism
Slide24Secondary and Tertiary Hypothyroidism
<1% hypothyroidism cases
Low or normal serum TSH concentrations + low serum T4 and T3
2
nd (TSH deficiency) hypothyroidism: - pituitary tumor - postpartum pituitary necrosis (Sheehan's syndrome) - trauma, infiltrative diseases.3rd (TRH deficiency) hypothyroidism can be caused by - Damages the hypothalamus or - Interferes with hypothalamic-pituitary portal blood flow
Slide25Medication Cause
Inhibit
GIT Absorption of thyroid hormone.
Separated by 4 hours
Slide26Screening and Its Importance
Slide27Overt hypothyroidism in pregnancy is rare
In continuing pregnancies hypothyroidism is associated with increased risk of:
Pre-
eclampsia
Placenta Abruptionincreased c-section ratesFetal death (especially if increased TSH occurs in 2nd trimester) Motherisk April 2007
Slide28More for the Baby!!
Maternal thyroid hormones are important in embryogenesis
No production until 12 weeks, therefore
needs mom’s T4 for fetal brain development
Maternal hypothyroidism can cause negative effect on fetal intellectual development. Higher incidence of LBW (due to medically indicated preterm delivery, pre-eclampsia, abruption)Iodine deficient hypothyroidism -> congenital cretinism (growth failure, mental retardation, other neuropsychological deficits) Motherisk April 2007, CMAJ Apr 2007 176(8)Treatment before 10 weeks’ gestation No adverse effect
Slide29Indications for Screening
universal
screening is
not recommended (ACOG)
Family Hx of autoimmune thyroid diseaseWomen on thyroid therapyPresence of goiter or thyroid nodulesHx of thyroid surgeryInfertilityUnexplained anemia or hyponatremia or high cholesterol levelPrevious Hx of - neck radiation - postpartum thyroid dysfunction - previous birth of infant with thyroid problemOther autoimmune chronic conditions: Type 1 DM
Slide30Laboratory Workup
Overt hypothyroidism:
symptomatic patient
elevated TSH level low levels of FT4 and FT3Subclinical hypothyroidism: asymptomatic patient elevated TSH normal FT4 and FT3
Slide31Treatment
Replacement with external thyroid hormone --
levothyroxine
(
Levothyroid, Levoxyl, Synthroid, and Unithroid). Levothyroxine (Synthroid) pregnancy category A A sterioisomer of physiologic thyroxine1.6 mcg/kg, usually about 50 to 100 mcg/day for women30-60 minutes before eating breakfast.
Slide32Treatment and Goals
The American Association of Clinical Endocrinologists recommends keeping the thyroid-stimulating hormone (TSH) level between
0.3 and 3.0 mIU/L.
After readjustment of levothyroxine, observe 6-8 weeks
Check TSH every trimester
Slide33Side Effects of L-Thyroxine :
Rapid or irregular heartbeat
Chest pain or shortness of breath
Muscle weakness Nervousness Irritability Sleeplessness
Tremors Change in appetite Weight loss
Slide34Pearls
Safe in pregnancy and lactation
Very little thyroxin crosses the placenta NO risk of thyrotoxicosis of fetusPatients who were on thyroxine therapy before pregnancy should increase the dose by 30% once pregnancy is confirmed (Bombrys et al, 2008) Keep TSH level between 0.3 and 3.0 mU/L.TSH should be monitored every trimester until delivery.
Slide35Overt hypothyroidism (OH)
OH complicates 2–10 per 1000 pregnancies and is commonly due to:
Hashimoto's thyroiditis
previous radioiodine therapy/thyroid surgeryprevious postpartum thyroiditishypopituitarism
iodine deficiency.
Slide36Maternal and fetal outcomes are worse with OH
higher risks of spontaneous miscarriage, PET,PIH, PPH & low birth weight.
There is a risk of a slight reduction in IQ in the fetus but no increased risk of congenital malformations.
Pregnancy itself probably has no effect on hypothyroidism although approximately 25% of women will require an increase in their thyroxine dose in pregnancy
Slide37Congenital cretinism
is a well-documented syndrome of growth restriction, deafness and neuropsychological impairment, resulting from severe iodine deficiency or untreated congenital hypothyroidism.
woman should be
euthryoid
at conception, on a stable dose of thyroxine and the importance of compliance during the first trimester should be emphasised.
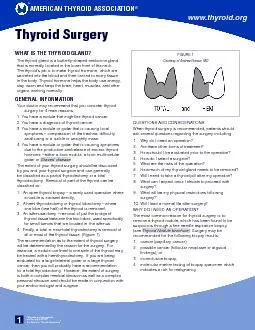
Slide38THANK YOU