
PRELead Purpose of Questionnaire To conduct a lead investigation while taking appropriate precautions due toCOVID19DATEinitial contactDATE Within24hrs of InvADDRESSProperty Event IDInitial Informat ID: 862616
Download Pdf The PPT/PDF document "Investigation Questionnaire for Family D..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






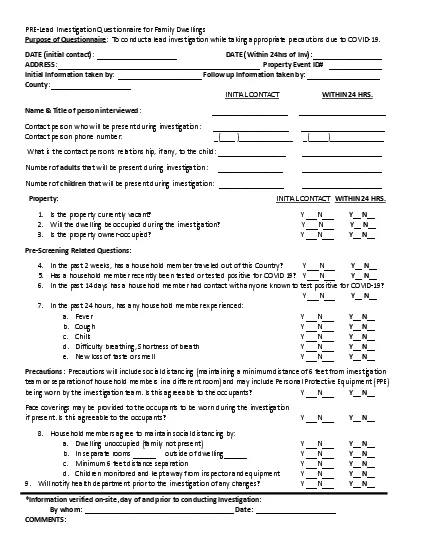
1 PRE - Lead Investigation Questionnaire
PRE - Lead Investigation Questionnaire for Family Dwellings Purpose of Questionnaire : To conduct a lead investigation while taking appropriate precautions due to COVID - 19. DATE (initial contact) : _____________________ DATE ( Within 24hr s of Inv ) : ______________ _ ___ ADDRESS : ______________________ _______________ _______________ _ Property Event ID# _ ___ _ _________ I nitial I nformation taken by : ______ __________ __ ___ _ Follow up Information taken by: __ ___ ______________ County : _____________________ INITIAL CONTACT WITHIN 24 HRS. Name & Title of person interviewed : ___ _________________ __ ______________ __ _____ Contact person who will be present during investigation : ____________________ _____________________ _ Contact person phone number: _ ( ____ ) ______________ _ ( _____ ) ______________ What is the contact person’s relations hip, if any, to the child : __________________ ________________ _ ____ Number of adults that will be present during investigation : ____ _ _ __ _ ________ ___ __________________ Number of children that will be present during investigation: _________________ _____________________ Property: INITIAL CONTACT WITHIN 24 HRS. 1. Is the property currently vacant? Y ___N___ Y__ N__ 2. Will the dwelling be occupied during the investigation? Y ___N___ Y__ N__ 3. Is the property owner - occupied? Y ___N___ Y__ N__ Pre - Screening Related Questions: 4. In the past 2 weeks, has a household member traveled out of this Count r y ? Y ___N___ Y__ N__ 5. Has a household member recently been tested or tested positive for COVID 19 ? Y ___N___ Y__ N__ 6. In the past 1 4 days has a household member had contact with any one known to test positive for COVID - 19? Y ___N___ Y__ N__ 7. In the past 24 hours, has any household member experienced: a. Fever Y ___N___ Y__ N__ b. Cough Y ___N___ Y__ N__ c. Chills Y ___N___ Y__ N__ d. Difficulty breathing , Shortness of breath Y ___N___ Y__ N__ e. New loss of taste or smell Y ___N___ Y__ N__ Precautions : Precautions will include s ocial d istancing ( maintaining a minimum distance of 6 feet from investigation team or separation of household members in a different room ) and may include Personal Protective Equipment (PPE) be ing worn by the investigation team . Is this agreeable to the occupants? Y ___N___ Y__ N__ Face coverings may be provided to the occupants to be worn during the investigation if present. Is this agreeable to the occupants? Y ___N___ Y__ N__ 8. H ousehold members agree to maintain s ocial d istancing by : a. Dwelling unoccupied (family not present) Y ___N___ Y__ N__ b. In separate rooms ___ _ __ outside of dwelling ______ Y ___N___ Y__ N__ c. Minimum 6 feet distance separation Y ___N___ Y__ N__ d. Children monitored and kept away from inspector and equipment Y ___N___ Y__ N__ 9. Will notify health department prior to the investigation of any changes ? Y ___N___ Y__ N__ * I nformation verified on - site , day of and prior to conducting Investigation: By whom: ___________________________________ ____ Date: _____________________ COMMENTS: