
D Amani Elgadal D efinition Measles is a highly contagious viral infection It is exanthematous disease with fever cough coryza rhinitis and conjunctivitis ID: 911672
Download Presentation The PPT/PDF document "Measles M orbilli, Rubeola, or red Me..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
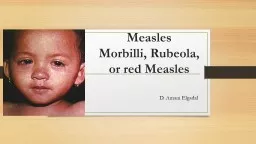
Measles Morbilli, Rubeola, or red Measles
D. Amani Elgadal
Slide2DefinitionMeasles is a highly contagious viral infection. It is exanthematous disease with fever, cough, coryza (rhinitis) and conjunctivitis. Before the widespread use of measles vaccines, it was estimated that measles caused between 5 million and 8 million deaths worldwide each year.
Slide3History of measlesThe first systematic description of measles, and its distinction from other exanthematous diseases (smallpox and chicken pox) is credited to the Persian physician Rhazes (860–932), who published : The Book of: Smallpox and Measles
Slide4In 1529, a measles outbreak in Cuba killed two thirds of those natives who had previously survived smallpox. Two years later, measles was responsible for the deaths of half the population of Honduras, Mexico, Central America and Inca civilizationMeasles killed 20 % of Hawaii's population in the 1850s. In 1875, measles killed over 40,000 Fijians, approximately one-third of the population
Slide5EtiologyMeasles is caused by Measles virus. Which is a spherical, single-stranded RNA virus with diameters of 100-250 nm. The family of Para myxoviridae. The genus of MorbillivirusThe virus was first isolated in 1954 by Nobel Laureate John F. Enders and Thomas Peebles
Slide6Although RNA viruses typically have high mutation rates, measles virus is considered to be an antigenically monotypic virus;Measles virus is killed by ultraviolet light and heat. The measles virus has two envelope glycoproteins on the viral surface— hemagglutinin (H) and membrane fusion protein (F). These proteins are responsible for host cell binding and invasion.
Slide7EPIDEMIOLOGY One of the most highly contagious directly transmitted pathogens.Outbreaks can occur in populations in which <10% of persons are susceptibleChains of transmission are household contacts, school-age children, and health care workers.There are
no latent or persistent infections that result in prolonged contagiousness, nor are there animal reservoirs
Slide8In temperate climates, annual measles outbreaks occur in the late winter and early spring. Transmission occurs 3-5 days before the rash. It remains communicable up to 4 days after the appearance of rush as the viral load in blood and body fluids is high.
Slide9Who are at risk? Unvaccinated young children • Unvaccinated pregnant women • Many developing countries – particularly in parts of Africa and Asia • Measles outbreaks can be particularly deadly • Interrupts routine immunization.
Slide10PATHOGENESIS It is an airborne disease through coughs and sneezes.It may also be spread through contact with saliva or nasal secretion in
the respiratory tract, oropharynx, or conjunctivae .
. • During the first 2–4 days after infection, measles virus proliferates locally in the respiratory mucosa and spreads to lymph nodes. •
Slide11Virus then enters to the bloodstream in infected leukocytes (primarily monocytes), producing the primary viremia that disseminates infection throughout the reticuloendothelial system. Further replication results in secondary viremia that begins 5–7 days after infection and disseminates measles virus throughout the body.
Slide12CLINICAL MANIFESTATIONS•Main symptoms Fever • Dry cough • Coryza • Sore throat • Inflamed eyes (conjunctivitis) • Koplik's spots (Tiny white spots with bluish-white centers on a red background) • A skin rash: maculopapular rash, hemorrhagic rash may occur
Slide13The Disease has 4 Phases• Incubation period (Phase) • Prodromal period (Phase) • Exanthema period (Phase) •
Convalescence period (Phase)
Slide14Incubation period (Phase):Is 8-10 days after exposed to the virus. During this period patient has no symptoms
Slide15Prodromal period (Phase):lasts 2-4 days and is marked by fever (39-40 C), malaise, cough, coryza, conjunctivitis and pharyngitisKoplik’s spots develop on the buccal mucosa during this phase, 2 days before the rash appears. Koplik’s spots seen inside the mouth are pathognomic (diagnostic) for measles, but are temporary and therefore rarely seen
Slide16Skin rash & conjunctivitis
Slide17Skin rash & conjunctivitis
Slide18Koplik’s spots
Slide19Koplik’s spots
Slide20Koplik's spotsKoplik’s spots are pathognomonic of measles and consist of bluish white dots ~1 mm in diameter surrounded by erythema.The lesions appear first on the buccal mucosa of the cheeks opposite the upper 1st & 2nd molars but rapidly increase in number to involve the entire buccal mucosa appears 2-3 days before the measles rash itself.
. They fade with the onset of rash.May appears in the lips
Slide21Differential diagnosis of Koplik's spots : Fordyce aphthae (which lack a bright red background). Aphthous ulcers (which are painful and less numerous), Parvovirus
B19 infection.
Slide22Exanthema period (Phase) Begins 2 weeks after exposure The maculopapular rash first appears behind the ears and on the neck. The rash progresses to cover face, trunk, arms, with involvement of the legs and feet within 72 h. The fever peaks on the 2nd or 3rd day of the rash. The rash usually begins to clear in the same order of progression as it appeared, usually beginning on the third or fourth day after onset.
Slide23Convalescence period (Phase) After 10-12 days Resolution of the rash may be followed by desquamation leaving transient hyper pigmented areas .
Slide24DIFFERENTIAL DIAGNOSISInclude other causes of fever, rash, and conjunctivitis, : • Rubella, • Kawasaki disease, • Infectious mononucleosis, • scarlet fever,
• Rocky Mountain spotted fever, • Enterovirus or adenovirus infection, • Drug sensitivity
Slide25DIAGNOSIS Easily diagnosed based on clinical symptoms particularly during outbreaks Koplik’s spots are especially helpful because they appear early and are pathognomonicCDC had case definition for measles:(1) a generalized maculopapular rash of at least 3 days’ duration; (2) fever of at least 38.3 o C
(3) cough, coryza, or conjunctivitis
Slide26Serology is the most common method of laboratory diagnosis. Detection of specific IgM in a single specimen of serum / oral fluid is considered diagnostic of acute infection. Also, a fourfold increase in measles specific IgG antibody levels between acute- and convalescent-phase in serum specimens.
Slide27Measles virus–specific IgM antibodies may not be detectable until 4–5 days or more after rash onset and usually fall to undetectable levels within 4–8 weeks of rash onsetMeasles also can be diagnosed by detection of measles virus RNA by reverse-transcriptase polymerase chain reaction (RT-PCR) from clinical specimens
Slide28TREATMENTThere is no specific antiviral therapy Treatment consists of general supportive measures, such as: • hydration • Bed rest • antipyreticTreat Secondary bacterial infections which are a major cause of morbidity and death following measles including
pneumonia and otitis media. Streptococcus pneumoniae and H. influenza type b are common pathogens.
Slide29Vitamin A is effective for the treatment of measles and can markedly reduce rates of morbidity and mortality.The World Health Organization recommends administration of once-daily doses of 200,000 IU of vitamin A for 2 consecutive days to all children with measles who are > 12 months of age. Lower doses are recommended for younger children: 100,000 IU per day for children 6–12 months of age and 50,000 IU per day for children <6 months old.
Slide30Complications Acute laryngo-tracheo bronchitis (croup) • Giant-cell pneumonitis • Secondary bacterial infections: Otitis media and bronchopneumonia • Central nervous system (SNS) complications: encephalomyelitis • subacute sclerosing pan encephalitis (SSPE)
Slide31Prevention Passive Immunization by specific Measles immunoglobulin • Active Immunization by Vaccine The recommended age of first vaccination varies from 6 to 15 months
Antibodies appear 12–15 days after vaccination and peak at 1–3 months. The vaccine-induced immunity persists several decades if not longer:
Slide32ProphylaxisPassive Immunization by specific Measles IG given shortly after exposure within 72 h can attenuate the clinical course of measles. Up to 6 days after exposure, IG can prevent or modify the disease. Prophylaxis with IG is recommended for susceptible household contacts at risk particularly children <1 year of age, immunocompromised persons (including HIV-infected persons) and pregnant women.