
1 Jeffrey Schachar MD 1 Trang Simon Christine Ahn MD 2 Wencheng Li MD 3 Catherine A Matthews MD 1 Robert J Evans MD 1 Gopal Badlani MD 1 Stephen J Walker PhD ID: 1040524
Download Presentation The PPT/PDF document "Raymond Xu MD 1 , Tyler Overholt MD" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



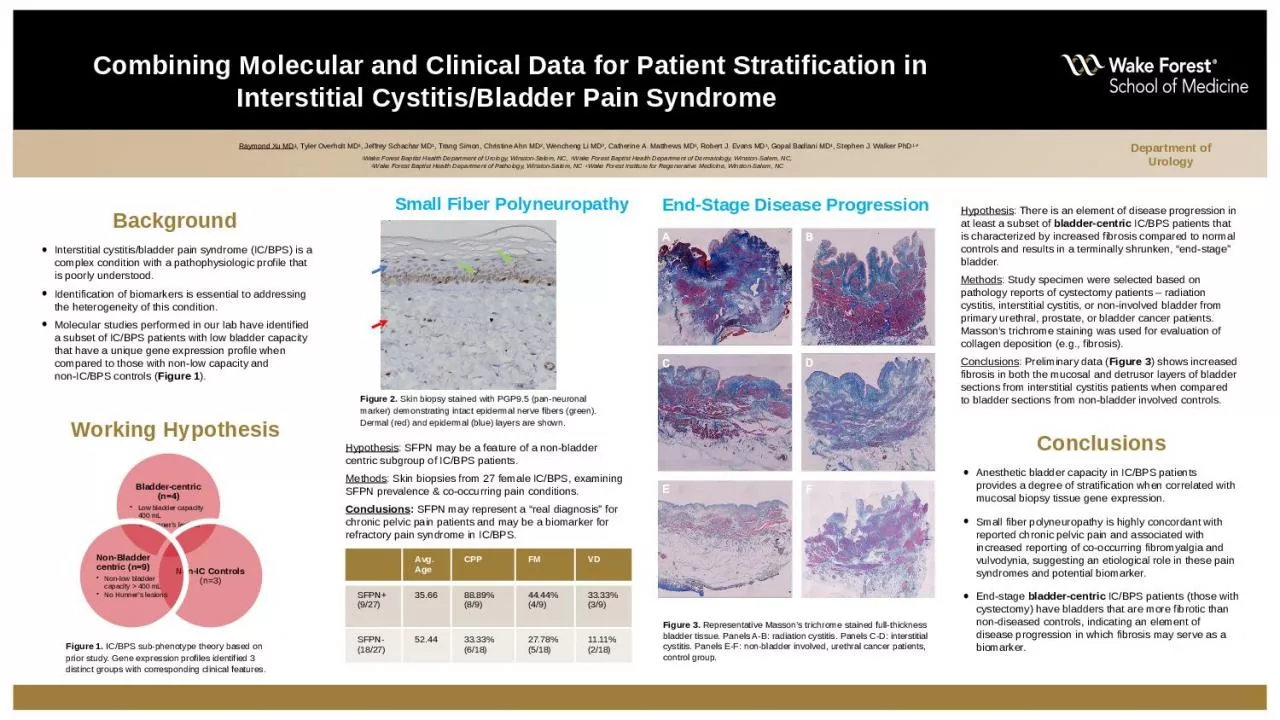
1. Raymond Xu MD1, Tyler Overholt MD1, Jeffrey Schachar MD1, Trang Simon, Christine Ahn MD2, Wencheng Li MD3, Catherine A. Matthews MD1, Robert J. Evans MD1, Gopal Badlani MD1, Stephen J. Walker PhD1,41Wake Forest Baptist Health Department of Urology, Winston-Salem, NC, 2Wake Forest Baptist Health Department of Dermatology, Winston-Salem, NC, 3Wake Forest Baptist Health Department of Pathology, Winston-Salem, NC 4Wake Forest Institute for Regenerative Medicine, Winston-Salem, NCCombining Molecular and Clinical Data for Patient Stratification in Interstitial Cystitis/Bladder Pain Syndrome BackgroundInterstitial cystitis/bladder pain syndrome (IC/BPS) is a complex condition with a pathophysiologic profile that is poorly understood. Identification of biomarkers is essential to addressing the heterogeneity of this condition.Molecular studies performed in our lab have identified a subset of IC/BPS patients with low bladder capacity that have a unique gene expression profile when compared to those with non-low capacity and non-IC/BPS controls (Figure 1).Department of UrologyWorking HypothesisConclusionsAnesthetic bladder capacity in IC/BPS patients provides a degree of stratification when correlated with mucosal biopsy tissue gene expression.Small fiber polyneuropathy is highly concordant with reported chronic pelvic pain and associated with increased reporting of co-occurring fibromyalgia and vulvodynia, suggesting an etiological role in these pain syndromes and potential biomarker.End-stage bladder-centric IC/BPS patients (those with cystectomy) have bladders that are more fibrotic than non-diseased controls, indicating an element of disease progression in which fibrosis may serve as a biomarker.Figure 1. IC/BPS sub-phenotype theory based on prior study. Gene expression profiles identified 3 distinct groups with corresponding clinical features.End-Stage Disease ProgressionSmall Fiber PolyneuropathyHypothesis: SFPN may be a feature of a non-bladder centric subgroup of IC/BPS patients.Methods: Skin biopsies from 27 female IC/BPS, examining SFPN prevalence & co-occurring pain conditions.Conclusions: SFPN may represent a “real diagnosis” for chronic pelvic pain patients and may be a biomarker for refractory pain syndrome in IC/BPS.Avg. AgeCPPFMVDSFPN+ (9/27)35.6688.89% (8/9)44.44% (4/9)33.33% (3/9)SFPN- (18/27)52.4433.33% (6/18)27.78% (5/18)11.11% (2/18)Figure 2. Skin biopsy stained with PGP9.5 (pan-neuronal marker) demonstrating intact epidermal nerve fibers (green). Dermal (red) and epidermal (blue) layers are shown.Figure 3. Representative Masson’s trichrome stained full-thickness bladder tissue. Panels A-B: radiation cystitis. Panels C-D: interstitial cystitis. Panels E-F: non-bladder involved, urethral cancer patients, control group.Hypothesis: There is an element of disease progression in at least a subset of bladder-centric IC/BPS patients that is characterized by increased fibrosis compared to normal controls and results in a terminally shrunken, “end-stage” bladder.Methods: Study specimen were selected based on pathology reports of cystectomy patients – radiation cystitis, interstitial cystitis, or non-involved bladder from primary urethral, prostate, or bladder cancer patients. Masson’s trichrome staining was used for evaluation of collagen deposition (e.g., fibrosis). Conclusions: Preliminary data (Figure 3) shows increased fibrosis in both the mucosal and detrusor layers of bladder sections from interstitial cystitis patients when compared to bladder sections from non-bladder involved controls.