
L Graham 12 7 R McConville 34 A Willis 5 S Napier 62 Honorary Specialty Registrar Oral and Maxillofacial PathologyICAT Fellow 1 Specialist Foundation Trainee 3 Oral Medicine Consultant ID: 1046825
Download Presentation The PPT/PDF document "A classic presentation of a rare cause o..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


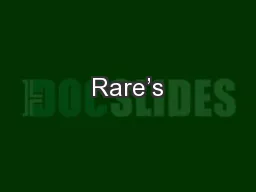

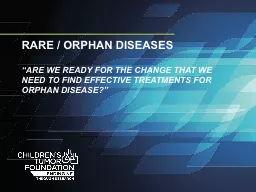
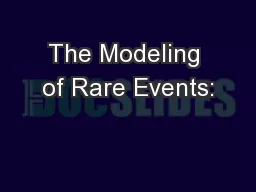


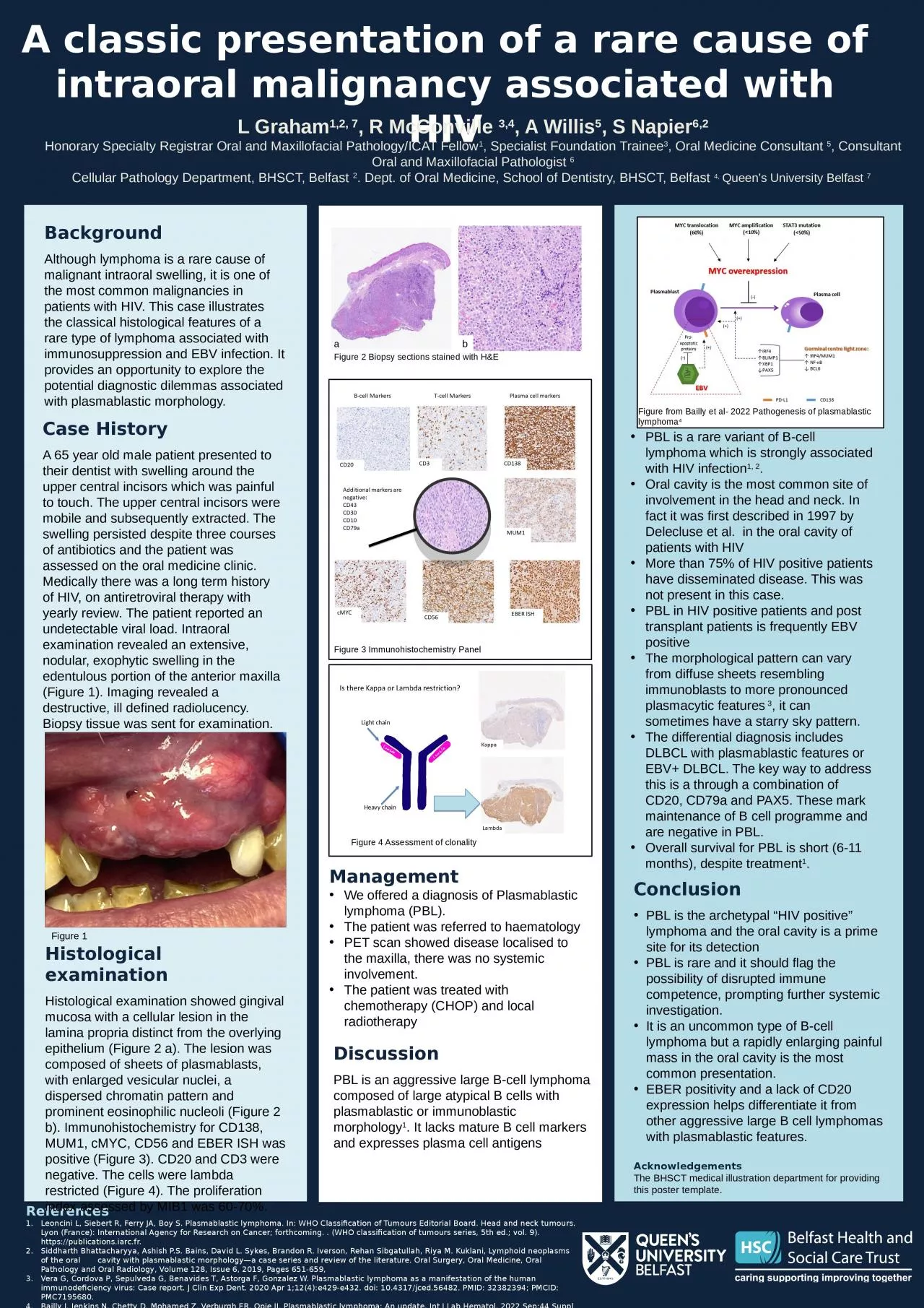
1. A classic presentation of a rare cause of intraoral malignancy associated with HIVL Graham1,2, 7, R McConville 3,4, A Willis5, S Napier6,2Honorary Specialty Registrar Oral and Maxillofacial Pathology/ICAT Fellow1, Specialist Foundation Trainee3, Oral Medicine Consultant 5, Consultant Oral and Maxillofacial Pathologist 6Cellular Pathology Department, BHSCT, Belfast 2. Dept. of Oral Medicine, School of Dentistry, BHSCT, Belfast 4, Queen’s University Belfast 7 References Leoncini L, Siebert R, Ferry JA, Boy S. Plasmablastic lymphoma. In: WHO Classification of Tumours Editorial Board. Head and neck tumours. Lyon (France): International Agency for Research on Cancer; forthcoming. . (WHO classification of tumours series, 5th ed.; vol. 9). https://publications.iarc.fr.Siddharth Bhattacharyya, Ashish P.S. Bains, David L. Sykes, Brandon R. Iverson, Rehan Sibgatullah, Riya M. Kuklani, Lymphoid neoplasms of the oral cavity with plasmablastic morphology—a case series and review of the literature. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, Volume 128, Issue 6, 2019, Pages 651-659,Vera G, Cordova P, Sepulveda G, Benavides T, Astorga F, Gonzalez W. Plasmablastic lymphoma as a manifestation of the human immunodeficiency virus: Case report. J Clin Exp Dent. 2020 Apr 1;12(4):e429-e432. doi: 10.4317/jced.56482. PMID: 32382394; PMCID: PMC7195680.Bailly J, Jenkins N, Chetty D, Mohamed Z, Verburgh ER, Opie JJ. Plasmablastic lymphoma: An update. Int J Lab Hematol. 2022 Sep;44 Suppl 1(Suppl 1):54-63. doi: 10.1111/ijlh.13863. Erratum in: Int J Lab Hematol. 2022 Dec;44(6):1121. PMID: 36074710; PMCID: PMC9545967.BackgroundAlthough lymphoma is a rare cause of malignant intraoral swelling, it is one of the most common malignancies in patients with HIV. This case illustrates the classical histological features of a rare type of lymphoma associated with immunosuppression and EBV infection. It provides an opportunity to explore the potential diagnostic dilemmas associated with plasmablastic morphology.Case HistoryA 65 year old male patient presented to their dentist with swelling around the upper central incisors which was painful to touch. The upper central incisors were mobile and subsequently extracted. The swelling persisted despite three courses of antibiotics and the patient was assessed on the oral medicine clinic. Medically there was a long term history of HIV, on antiretroviral therapy with yearly review. The patient reported an undetectable viral load. Intraoral examination revealed an extensive, nodular, exophytic swelling in the edentulous portion of the anterior maxilla (Figure 1). Imaging revealed a destructive, ill defined radiolucency. Biopsy tissue was sent for examination. PBL is a rare variant of B-cell lymphoma which is strongly associated with HIV infection1, 2. Oral cavity is the most common site of involvement in the head and neck. In fact it was first described in 1997 by Delecluse et al. in the oral cavity of patients with HIVMore than 75% of HIV positive patients have disseminated disease. This was not present in this case.PBL in HIV positive patients and post transplant patients is frequently EBV positive The morphological pattern can vary from diffuse sheets resembling immunoblasts to more pronounced plasmacytic features 3, it can sometimes have a starry sky pattern.The differential diagnosis includes DLBCL with plasmablastic features or EBV+ DLBCL. The key way to address this is a through a combination of CD20, CD79a and PAX5. These mark maintenance of B cell programme and are negative in PBL.Overall survival for PBL is short (6-11 months), despite treatment1.ConclusionPBL is the archetypal “HIV positive” lymphoma and the oral cavity is a prime site for its detectionPBL is rare and it should flag the possibility of disrupted immune competence, prompting further systemic investigation. It is an uncommon type of B-cell lymphoma but a rapidly enlarging painful mass in the oral cavity is the most common presentation. EBER positivity and a lack of CD20 expression helps differentiate it from other aggressive large B cell lymphomas with plasmablastic features.AcknowledgementsThe BHSCT medical illustration department for providing this poster template.Figure 2 Biopsy sections stained with H&EabFigure 1Histological examinationHistological examination showed gingival mucosa with a cellular lesion in the lamina propria distinct from the overlying epithelium (Figure 2 a). The lesion was composed of sheets of plasmablasts, with enlarged vesicular nuclei, a dispersed chromatin pattern and prominent eosinophilic nucleoli (Figure 2 b). Immunohistochemistry for CD138, MUM1, cMYC, CD56 and EBER ISH was positive (Figure 3). CD20 and CD3 were negative. The cells were lambda restricted (Figure 4). The proliferation index assessed by MIB1 was 60-70%. ManagementWe offered a diagnosis of Plasmablastic lymphoma (PBL).The patient was referred to haematologyPET scan showed disease localised to the maxilla, there was no systemic involvement.The patient was treated with chemotherapy (CHOP) and local radiotherapyFigure 3 Immunohistochemistry PanelDiscussionPBL is an aggressive large B-cell lymphoma composed of large atypical B cells with plasmablastic or immunoblastic morphology1. It lacks mature B cell markers and expresses plasma cell antigens Figure 4 Assessment of clonalityHeavy chainLight chainFigure from Bailly et al- 2022 Pathogenesis of plasmablastic lymphoma4