
Rachael Rzasa Lynn MD Chronic Pain Zoom Webinar 2 December 2015 Definitions Most basic neurophysiologic classification based on presumed mechanism of pain Simplified there are 2 types of pain ID: 633075
Download Presentation The PPT/PDF document "Pain Classification: Nociceptive, Neurop..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
Pain Classification:Nociceptive, Neuropathic, Central and Mixed
Rachael Rzasa Lynn, MD
Chronic Pain Zoom Webinar
2 December 2015Slide2
Definitions
Most basic = neurophysiologic classification
based
on
presumed mechanism
of pain.
Simplified, there are 2 types of pain:
nociceptive pain
non
-nociceptive
pain
Neuropathic pain
Idiopathic pain
≠psychogenic pain!Slide3
Nociceptive Pain
Pain due to continuous tissue injury
actual or threatened damage to non-neural tissue results in activation of peripheral
nociceptors
noxious
stimulus electrochemical impulses in peripheral nerves spinal cord brain= transduction, transmission, modulation, and perceptionExamples: arthritis pain, acute post-traumatic painSubdivided into somatic pain and visceral pain
Basbaum
et al.
Cell
2009; 139:
267-284Slide4
Nociceptive Pain
Somatic pain
excitation and/or sensitization
of
nociceptors
in tissues such as bone, periarticular soft tissue, joints, and muscles Well localizedIntermittent or constant“aching,” “stabbing,” “gnawing,” “throbbing”Slide5
Nociceptive Pain
Visceral pain
Not produced by all
visceral
organs
Liver, kidney, most solid viscera, and lung parenchyma are not sensitive to pain.Not always created by visceral injury Cutting intestine causes no pain, stretching of the bladder is painfulDiffuse and poorly localizedNo separate visceral sensory pathway and low proportion of afferent nerve fibers from visceraIntermittent or constant“dull,” “colicky,” “squeezing”Referrs to other
locations.Accompanied by motor and autonomic reflexes
Eg
, nausea
, vomiting,
muscle tension, etc.Slide6
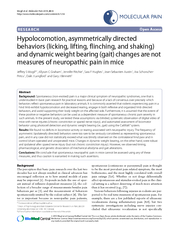
Neuropathic Pain
“Pain
arising as a direct consequence of a lesion or disease affecting the somatosensory system
.”
at
any point(s) within the somatosensory pathwaysPain from lesion/disease sustained by aberrant processing in the peripheral and/or central nervous systemtypically described as “sharp” or “burning”This is a clinical description (NOT a diagnosis) According to IASP,“this requires a demonstrable lesion or a disease that satisfies established neurological diagnostic criteria.”“The presence of symptoms or signs (e.g., touch-evoked pain) alone does not justify the use of the term
neuropathic.”“It is
common…that
diagnostic testing may yield inconclusive or even inconsistent data. In such instances, clinical judgment is required to reduce the totality of findings in a patient into one putative diagnosis or concise group of diagnoses
.”Slide7
Neuropathic Pain
Subsets
Peripherally
generated pain:
involves such
cervical or lumbar radiculopathy, spinal nerve lesions, and brachial or lumbosacral plexopathiesCentrally generated pain:involves injury to the central nervous system at the level of the spinal cord or above. Sympathetically maintained pain:may be generated peripherally or centrallycharacterized by localized autonomic dysregulationvasomotor or sudomotor changes, edema, sweating, trophic changes including atrophyComplex Regional Pain SyndromeSlide8
Central Pain States
Central pain
: Pain initiated or caused by a primary lesion or dysfunction in the central nervous system.
Can be produced by an type of vascular
, demyelinating, infectious, inflammatory, or traumatic lesion in the
brain or spinal cordEg, post-stroke painCentral sensitization: Increase in the excitability of neurons in the spinal cord.Increased responsiveness of nociceptive neurons in the central nervous systemIncreased response to input to which they normally respondActivation in response to subthreshold inputSlide9
IASP Pain Classification
Multidimensional
Classification of
Pain
Developed to standardize descriptions of pain syndromes and provide a point of reference
Uses 5 axes to classify chronic painRegion of the body affected (Axis I),System whose abnormal functioning could produce the pain (Axis II),Temporal characteristics of pain and pattern of occurrence (Axis III),Patient's statement of intensity and time since onset of pain (Axis IV)Mild, medium or severe, each for ≤1 month, 1-6 months or >6 months durationPresumed Etiology (Axis V
)Infection, inflammation, neoplasm, toxic, metabolic, etc
Uses the above to create 5-digit code assigned to each chronic pain diagnosis
Limitations: Does not include psychosocial or behavioral data
ALL PAIN HAS A PSYCHOLOGICAL COMPONENTSlide10
Proposed Taxonomy of Pain Based upon Multifactorial Assessment
Pain
Parameters:
Anatomy/System
Duration/Intensity/Quality
Associated Abnormality (physical/psychological)Underlying Diseases:Signs/SymptomsPain Mechanisms:NEUROPHYSIOLOGICALPrimary afferent involvementCNS involvementPSYCHOLOGICALCognitive-Affective-Behavioral InvolvementCognitive appraisal of painCoping
Affect/moodEnvironment Slide11
Mixed Pain
Most pain is mixed
Even “nociceptive pain” can lead to central sensitization
Eg
, osteoarthritis
fMRI and PET changesIncreased activation in brain areas involved with affect, aversive conditioning and motivation than experimental painThese patients display hyperalgesia locally and in areas distant from the arthritic jointAfter THA, these patients display reduced pain in both areasALL pain has a psychological component!
Aranda
-Villalobos P et al. Arthritis & Rheumatism 2013; 65:
1262-1270.
Sofat
et al.
Rheumatology
2011; 50:
2157-2165Slide12
TRP: Transient
receptor potential
channel (many subtypes)
TRPA1=cold
(<15°C) in injury (not normal, acute cold), menthol TRPM8=cold(<25°C), menthol TRPV1=heat (>43°C), capsaicinASICs: Acid-sensing ion channelsKCNK: Potassium channel subtypesNav: Voltage-gated sodium channel isoformsAlso Voltage-gated Calcium channels (N- and T-type); α2δ subunit ↑’d after injury Mechanical transduction may occur via TRP, ASIC and/or KCNK channels
Grace PM, et al.
Nat Rev
Immunol
.
2014;
14: 217-
231
Basbaum
et al. Cell 2009; 139: 267-284Slide13
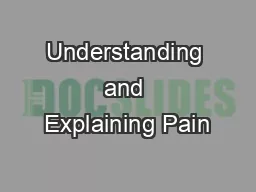
Mechanistic Stratification of Medications Used
to Treat Neuropathic Pain
Fig. 4. Mechanistic stratification of antineuralgic agents. PNS = peripheral nervous system; CBZ = carbamazepine; OXC = oxcarbazepine; PHT = phenytoin; TPM = topiramate; LTG = lamotrigine; TCA = tricyclic antidepressant; NE = norepinephrine; SSRI = selective serotonin re-uptake inhibitor; SNRI = serotonin and norepinephrine re-uptake inhibitor; GBP = gabapentin; LVT = levetiracetam; NMDA = N-methyl-D-aspartate; NSAID = nonsteroidal anti-inflammatory drug.
Beydouna
&
Backonja
M.
J Pain Symptom Manage.
2003;25:S18-30