
Regularity regular normal 010 s P waves PR interval 012 s QRS duration Interpretation Sinus Bradycardia Sinus Bradycardia Deviation from NSR Rate lt 60 bpm 4 ID: 912380
Download Presentation The PPT/PDF document "1 Rhythm #1 3 30 bpm Rate?" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
1
Slide2Slide3Rhythm #1
3
30 bpm
Rate?
Regularity?
regular
normal
0.10 s
P waves?
PR interval?
0.12 s
QRS duration?
Interpretation?
Sinus Bradycardia
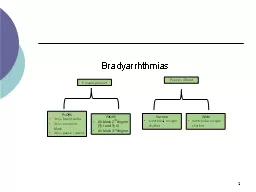
Slide4Sinus Bradycardia
Deviation from NSR
- Rate
< 60 bpm
4
Slide5Sinus Bradycardia
Etiology:
SA node is depolarizing slower than normal, impulse is conducted normally (i.e. normal PR and QRS interval).
5
Slide6Rhythm #2
6
130 bpm
Rate?
Regularity?
regular
normal
0.08 s
P waves?
PR interval?
0.16 s
QRS duration?
Interpretation?
Sinus Tachycardia
Slide7Rhythm #3 :Sinus Tachycardia
Deviation from NSR
- Rate
> 100 bpm
7
Slide8Sinus Tachycardia
Etiology:
SA node is depolarizing faster than normal, impulse is conducted normally.
Remember: sinus tachycardia is a response to physical or psychological stress, not a primary arrhythmia.
8
Slide9Rhythm 3 :Sinus Arrest
Etiology:
SA node fails to depolarize and no compensatory mechanisms take over
Sinus arrest is usually a transient pause in sinus node activity
9
Slide10Premature Beats
Premature Atrial Contractions
(PACs)
Premature Ventricular Contractions
(PVCs)
10
Slide11Premature Atrial Contraction
11
70 bpm
Rate?
Regularity?
occasionally irreg.
2/7 different contour
0.08 s
P waves?
PR interval?
0.14 s (except 2/7)
QRS duration?
Interpretation?
NSR with Premature Atrial Contractions
Slide12Premature Atrial Contractions
Deviation from NSR
These ectopic beats originate in the atria (but not in the SA node), therefore the contour of the P wave, the PR interval, and the timing are different than a normally generated pulse from the SA node.
12
Slide13Premature Atrial Contractions
Etiology:
Excitation of an atrial cell forms an impulse that is then conducted normally through the AV node and ventricles.
13
Slide14Teaching Moment
When an impulse originates anywhere in the atria (SA node, atrial cells, AV node, Bundle of His) and then is conducted normally through the ventricles, the QRS will be narrow (0.04 - 0.12 s).
14
Slide15Rhythm #4
15
60 bpm
Rate?
Regularity?
occasionally irreg.
none for 7
th
QRS
0.08 s (7th wide)
P waves?
PR interval?
0.14 s
QRS duration?
Interpretation?
Sinus Rhythm with 1 PVC
Slide16PVCs
Deviation from NSR
Ectopic beats originate in the ventricles resulting in wide and bizarre QRS complexes.
When there are more than 1 premature beats and look alike, they are called “uniform”. When they look different, they are called “multiform”.
16
Slide17PVCs
Etiology:
One or more ventricular cells are depolarizing and the impulses are abnormally conducting through the ventricles.
17
Slide18Teaching Moment
When an impulse originates in a ventricle, conduction through the ventricles will be inefficient and the QRS will be wide and bizarre.
18
Slide19Ventricular Conduction
19
Normal
Signal moves rapidly through the ventricles
Abnormal
Signal moves slowly through the ventricles
Slide20Supraventricular Arrhythmias
Atrial Fibrillation
Atrial Flutter
Paroxysmal Supra Ventricular Tachycardia (PSVT)
20
Slide21Rhythm #5
21
100 bpm
Rate?
Regularity?
irregularly irregular
none
0.06 s
P waves?
PR interval?
none
QRS duration?
Interpretation?
Atrial Fibrillation
Slide22Atrial Fibrillation
Deviation from NSR
No organized atrial depolarization, so no normal P waves (impulses are not originating from the sinus node).
Atrial activity is chaotic (resulting in an irregularly irregular rate).
Common, affects 2-4%, up to 5-10% if > 80 years old
22
Slide23Atrial Fibrillation
Etiology:
due to multiple re-entrant wavelets conducted between the R & L atria and the impulses are formed in a totally unpredictable fashion.
The AV node allows some of the impulses to pass through at variable intervals (so rhythm is irregularly irregular).
23
Slide24Rhythm #6
24
70 bpm
Rate?
Regularity?
regular
flutter waves
0.06 s
P waves?
PR interval?
none
QRS duration?
Interpretation?
Atrial Flutter
Slide25Atrial Flutter
Deviation from NSR
No P waves. Instead flutter waves (note “sawtooth” pattern) are formed at a rate of 250 - 350 bpm.
Only some impulses conduct through the AV node (usually every other impulse).
25
Slide26Atrial Flutter
Etiology:
Reentrant pathway in the right atrium with every 2nd, 3rd or 4th impulse generating a QRS (others are blocked in the AV node as the node repolarizes).
26
Slide27Rhythm #7
27
74
148
bpm
Rate?
Regularity?
Regular
regular
Normal
none
0.08 s
P waves?
PR interval?
0.16 s
none QRS duration?
Interpretation?
Paroxysmal Supraventricular Tachycardia
(PSVT)
Slide28PSVT:Paroxysmal
S
upra
V
entricular
TachycardiaDeviation from NSR
The heart rate suddenly speeds up, often triggered by a PAC (not seen here) and the P waves are lost.
28
Slide2929
Rhythm 8: Ventricular Tachycardia
Ventricular cells fire continuously due to a looping re-entrant circuit
Rate usually regular, 100 - 250 bpm
P wave: may be absent, inverted or retrograde
QRS: complexes bizarre, > .12
Rhythm: usually regular
Slide3030
Slide3131
Rhythm 9: Ventricular Fibrillation
Rhythm: irregular-coarse or fine, wave form varies in size and shape
Fires continuously from multiple foci
No organized electrical activity
No cardiac output
Causes: MI, ischemia, untreated VT, underlying CAD, acid base imbalance, electrolyte imbalance, hypothermia,
Slide32AV Nodal Blocks
1st Degree AV Block
2nd Degree AV Block, Type I
2nd Degree AV Block, Type II
3rd Degree AV Block
32
Slide33Rhythm #10
33
60 bpm
Rate?
Regularity?
regular
normal
0.08 s
P waves?
PR interval?
0.36 s
QRS duration?
Interpretation?
1st Degree AV Block
Slide341st Degree AV Block
Deviation from NSR
PR Interval
> 0.20 s
34
Slide351st Degree AV Block
Etiology:
Prolonged conduction delay in the AV node or Bundle of His.
35
Slide36Rhythm #11
36
50 bpm
Rate?
Regularity?
regularly irregular
nl, but 4th no QRS
0.08 s
P waves?
PR interval?
lengthens
QRS duration?
Interpretation?
2nd Degree AV Block, Type I
Slide372nd Degree AV Block, Type I
Deviation from NSR
PR interval progressively lengthens, then the impulse is completely blocked (P wave not followed by QRS).
37
Slide382nd Degree AV Block, Type I
Etiology:
Each successive atrial impulse encounters a longer and longer delay in the AV node until one impulse (usually the 3rd or 4th) fails to make it through the AV node.
38
Slide39Rhythm #12
39
40 bpm
Rate?
Regularity?
regular
nl, 2 of 3 no QRS
0.08 s
P waves?
PR interval?
0.14 s
QRS duration?
Interpretation?
2nd Degree AV Block, Type II
Slide4040
2nd Degree AV Block, Type II
Deviation from NSR
Occasional P waves are completely blocked (P wave not followed by QRS).
Slide4141
Rhythm #13
40 bpm
Rate?
Regularity?
regular
no relation to QRS
wide (> 0.12 s)
P waves?
PR interval?
none
QRS duration?
Interpretation?
3rd Degree AV Block
Slide4242
3rd Degree AV Block
Deviation from NSR
The P waves are completely blocked in the AV junction; QRS complexes originate independently from below the junction.
Slide4343
3rd Degree AV Block
Etiology:
There is complete block of conduction in the AV junction, so the atria and ventricles form impulses independently of each other.
Without impulses from the atria, the ventricles own intrinsic pacemaker kicks in at around 30 - 45 beats/minute.
Slide4444
Remember
When an impulse originates in a ventricle, conduction through the ventricles will be inefficient and the QRS will be wide and bizarre.
Slide4545
Rhythm 14 :
Asystole
Ventricular standstill, no electrical activity, no cardiac output – no pulse!
Cardiac arrest, may follow VF or PEA
Rate: absent due to absence of ventricular activity. Occasional P wave may be identified.
Slide4646
Rhythm 15 :
IdioVentricular
Rhythm
Escape rhythm (safety mechanism) to prevent ventricular standstill
HIS/purkinje
system takes over as the heart’s pacemakerTreatment: pacingRhythm: regularRate: 20-40 bpmP wave: absentQRS: > .12 seconds (wide and bizarre)
Slide47QUESTIONS???