
3 CHEERS OREWORD the mental health of the general population For too long mental health has been mysterious to 145ordinary146 people and is seldom talked about in comparison to many areas of ID: 954641
Download Pdf The PPT/PDF document "Each year the Mental Health Foundation u..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.








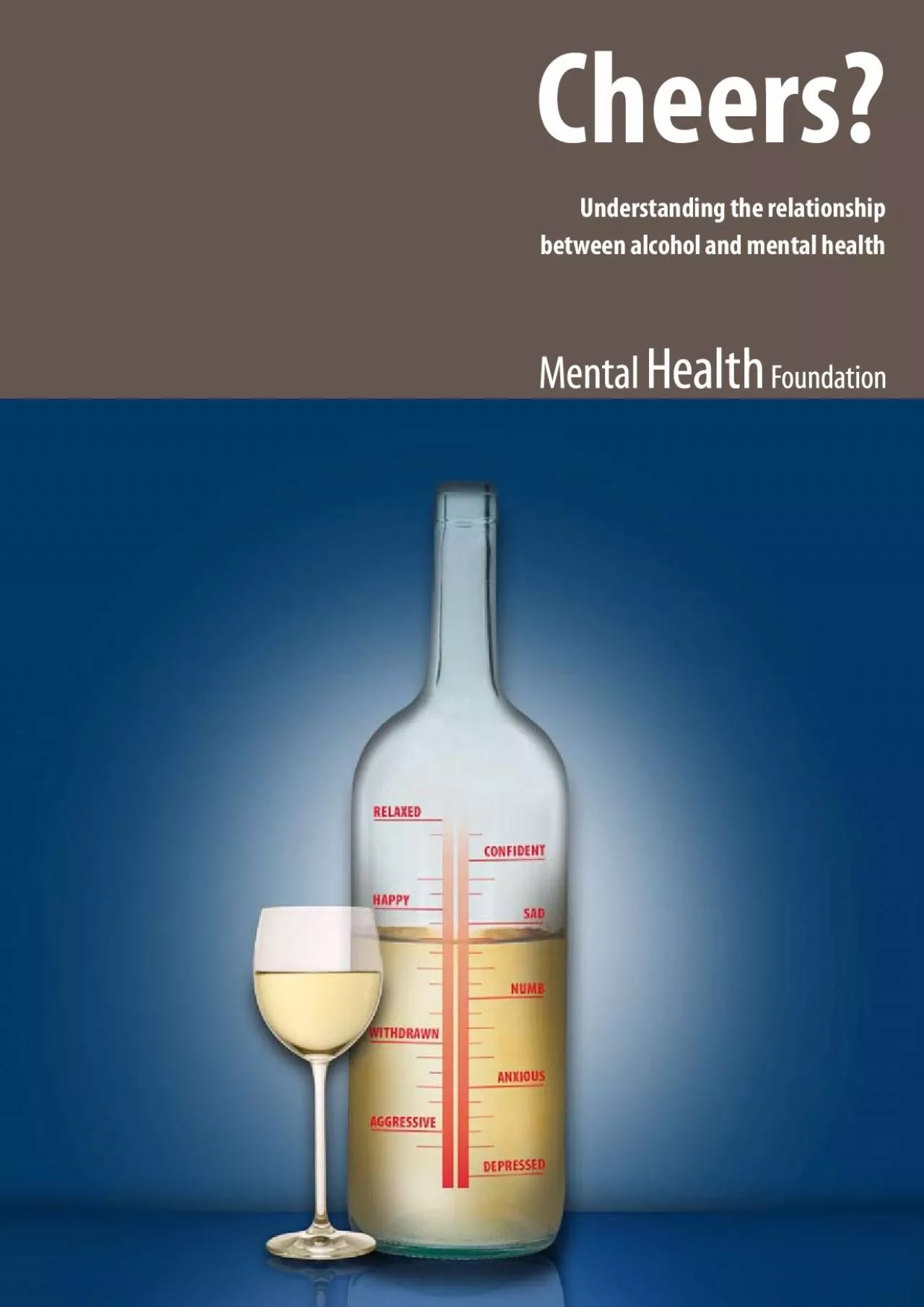
3 CHEERS? OREWORD Each year the Mental Health Foundation uses mental health action week to highlight an area of concern about the mental health of the general population. For too long mental health has been mysterious to ‘ordinary’ people, and is seldom talked about in comparison to many areas of physical health. Yet one in four of us will experience a mental health problem each year. The need for mental health to be demysti ed is urgent. We have been working for many years to give ordinary people the informa
tion they need to better understand their own – and others’ mental health. Recently we have covered practical topics such as the importance of diet and exercise to mental health, and the su ering caused to ordinary people with mental health problems because of the prejudice and ignorance surrounding mental illness. The message is clear – mental health is everyone’s business, just like physical health. As a society we must get better at understanding mental health, if we are to tackle some of the ma
jor health, economic and social burdens that face current and future generations. One of the least explored but most fundamentally important factors in the mental health of the general population is our use of alcohol. While much debate has taken place recently about alcohol, we have failed to draw out the reasons why so many people have troubled relationships with alcohol. The reasons we drink and the consequences of excessive drinking are intimately linked with our mental health, and this holds the key to dealing with
growing worries about alcohol misuse. But once again, mental health is swept under the carpet while debate focuses on the physical consequences of alcohol misuse. While this is just one example of how mental health is a crucial factor that is omitted from virtually every national debate, it is a vitally important one, and I am pleased that our research will add to the evidence. We hope it will spark and inform further debate, and o er useful directions to those who are rightly concerned. Dr Andrew McCulloch Chief Exec
utive Mental Health Foundation 1 CHEERS? GUE 2: CHACTERISOFOPLE PORING TAT AOHOLEESSINHITE 0 10 20 30 40 50 60 70 80 Drink right amount Drink too much Drink 5-6x per wk Drink 1x per wk Not working Full time work Class DE Class AB Over 65s 25-44 yr old Percentage of respondents Approximately one third of the sample report that drinking makes them feel less anxious (40%), less depressed (26%) and more able to forget problems (30%). This is consistent with the theory that people use alcohol to medicate low levels of stress, a
nxiety and depression. It is also consistent with the argument that using alcohol to self-medicate can lead to cyclical patterns of drinking – those who report using alcohol to cope with anxiety and depression are those who are drinking nearly every day and also think they would have di culty giving up (see Figures 3 & 4). Why do people drink alcohol? 1 CHEERS? Respondents were asked if they thought they drank too much, too little or about the right amount. Roughly equal numbers of people reported that they dran
k too much or too little, whilst the remaining two thirds considered that they drank about the right amount (see Figure 6). Those who thought they drank too much tended to be 7% of males, compared to 0% of females), younger (25% of 8-24 year olds, compared with 2% of over 65s), single (20% of single people, compared to % of married people) and in full time work (5%, compared to 8% of those not working). Nearly half of those drinking 5-6 times each week reported that they were drinking too much (compared to under 5% of thos
e drinking less than once a week) and over one third of those who thought they were drinking too much say they would nd it di cult to give up. GUE 6: RESPOND’ CEIONS ABUT TE AMOT OF AOHOL Why do people drink alcohol? This data supports the evidence found in the literature. Older people tend to drink more frequently, but drink smaller amounts, which they don’t think they would nd di cult to give up, whereas younger people tend to drink less often but consume more, recognise they drink too much an
d report that they would nd it di cult to give up. Because respondents weren’t asked about the amount they drank, it is hard to determine the number of people drinking above the recommended daily benchmarks of 3 units for women and 4 units for men. However, one quarter of those aged 8-24 and nearly half of those drinking 5-6 times per week say that they are drinking too much (and people tend to underestimate the amount they drink). This points to the need for e ective and accessible alternatives to drink
ing, especially where it is being used to alleviate symptoms of anxiety, depression or social inhibition. 0 10 20 30 40 50 60 70 80 Right amount Too little Too much Percentage of respondents 22 CHEERS? THE ASSOCIATIONBETWEENCOHOL USEANDSPECIFICMENTAL HEATHPROBEMS o-existence of mental health problems and alcohol use That some people experience problems both with their mental health and with their use of alcohol is not a new phenomenon. The concept of ‘dual-diagnosis’ has gained prominence in the last couple of de
cades, due in part to the closure of large psychiatric hospitals and to the increasing prevalence of alcohol and drug misuse and dependency in the population 39 . The terminology is debated amongst researchers and practitioners because of its implications that there are only two diagnoses involved, when in fact individuals often have a cluster of complex and inter-related needs . This is re ected in the di erent ways the problems may occur 39 : alcohol use (even small amounts for some people) may lead to psychiatr
ic symptoms dependence on alcohol (“needing” a drink to get through an occasion or to relieve a negative emotional state) may produce psychological symptoms intoxication may result in short-term behavioural or psychological problems withdrawal or detoxi cation from alcohol may lead to psychological or psychiatric symptoms alcohol use may exacerbate a pre-existing mental health problem pre-existing mental health problems may lead to increased alcohol use There are many factors that contribute to a person’s
mental health and wellbeing and few research studies try to o er a simple causal relationship between alcohol use and mental health. Instead, much of the research has focused on the extent of the overlap between mental ill health and problem drinking, and the data is striking. The hospital admissions with a primary or secondary diagnosis of “mental and behavioural disorders due to alcohol” rose from 7995/96 to over 90,000 in 2002/035 and many GPs believe that alcohol is a causal factor in mental health probl
ems 42 . Research in the USA has suggested that the prevalence of alcohol dependence in those with psychiatric disorders is almost twice as high as in the general population and similar levels are reported for the U 43 . Similarly, research shows that people with alcohol dependency are more at risk of suicide 44 , have higher levels of depressive and a ective problems, schizophrenia and personality disorders 39 . There has been much research exploring the association between alcohol use and these speci c mental he
alth issues and some of the ndings are summarised below. 4.2 Suicide In 995, there were 5,095 suicides in the U and although there has been a small overall decline in the last decade, suicide still accounts for about 00,000 women 45 . The estimated risk of suicide in the presence of current alcohol misuse or dependence is eight times greater than in the absence of current alcohol misuse or dependence 6 . As many as 65% of suicides have been linked to excessive drinking 44 and alcohol problems are one of the highes
t risk factors for suicides, especially amongst males. Up to 40% of men who try to kill themselves have had a long-standing problem with alcohol and as many as 70% of those who succeed have drunk alcohol before doing so 3 . In one Northern Ireland suicide study, it was found that the prevalence of alcohol use disorders among people who committed suicide was 43% 46 . A further study 04 gunshot suicides in Northern Ireland over a 5-year period found that alcohol consumption was involved 47 . A study conducted among women in
a general hospital ward found that excessive alcohol consumption was signi cantly associated with attempted suicide by drug overdose 48 . • • • • • • 23 CHEERS? The Association between alcohol use and speci c mental health problems Young people are also particularly vulnerable and there is a strong empirical link between alcohol use and suicidal ideation, suicidal attempts and completed suicides amongst people under the age of 24 . In 2002, 75-24 year committed suicide, with many th
ousands more contemplating or attempting it 50 and it is estimated that one third of suicides amongst young people are committed whilst the young person is intoxicated . Young men are particularly at risk: suicide is the biggest single killer of young men aged under 35 in the United . In 2002 there were 5,882 suicides of which 5 were young men between the ages of opposed to 380 women between the same ages 52 . One explanation for this di erence in rates between young men and women is that whilst risk factors such as
unemployment, homelessness, family background and substance abuse a ect both men and women, men may not reach out for help or support in the same way that women might 52 . Alcohol use has also been associated with increased risk of unintentional injury and increased risk taking behaviours, which can have negative consequences for physical and mental health. These include drink-driving, violence, increased vulnerability to assault, falls, res, domestic violence and tra c accidents (vehicles, bicycles, and pe
destrians) 6 . This may be a consequence of the e ect of alcohol on the serotonin (5HT) and GABA brain receptors that may reduce fear and anxiety about social, physical or legal consequences of one’s actions. Alcohol also a ects cognitive functioning 53 , leading to impaired problem solving in con ict situations 54 and overly emotional responses or emotional ability 55 . Both suicide and risk-taking behaviours are correlated with other risk factors. In particular, they have been associated with other ps
ychological and psychiatric conditions, including depression, anxiety and personality disorders 49;56-58 . 4.3 Depression & nxiety At least two thirds of alcohol-dependent individuals entering treatment show evidence of anxiety, sadness, depression and/or manic-like symptoms . Over a 2-month and lifetime basis, alcohol dependence and major depression co-occur in the general population at levels higher than chance . Similarly, amongst those in the general population who drink alcohol, higher volume of consumption is associ
ated with more symptoms of depression 62 . Among patients in treatment for alcohol abuse and dependence, the prevalence of major depression is higher than in the general population 60;63-66 . Higher prevalence of alcohol use disorders has been documented for patients in treatment for depression 67;68 . Collectively, this evidence base suggests that alcohol use disorders are linked to depressive symptoms, and that alcohol dependence and depressive disorders co-occur to a larger degree than expected by chance. However, it
is not clear in the individual case whether the depression causes alcohol problems, whether the alcohol consumption or alcohol problems caused depression, or whether both could be attributed to a third cause 69 . Because depression is a multi-faceted experience, it is likely that alcohol problems and depression interact with a number of other factors that maintain or worsen depressive symptoms. It is also likely that risk factors for poor mental health are also risk factors for alcohol misuse. As we saw earlier, self-medi
cation has been proposed as an explanation for alcohol consumption in people with non-clinical levels of anxiety and depression. It can also o er an explanation for people with more severe levels of depression. As increased tolerance leads to increased drinking, the individual is left needing more alcohol to achieve the same e ect. The pharmacological actions of alcohol can also interact with an individual’s pre-existing mood or personality, the drinker’s beliefs and expectations about the e ect of t
he alcohol and the context in which it is being consumed 43 . Thus drinking may intensify and reinforce the feelings of the person drinking alcohol, exacerbating the cyclical pattern described earlier. 24 CHEERS? Su cient evidence now exists to assume alcohol’s contributory role in depression 6 . For example, in some countries, onset of depression follows onset of alcohol misuse, pointing to the likelihood that alcohol exacerbates underlying or previously undetected depression 70 . In addition, there is some ev
idence that abstaining from drinking signi cantly reduces depressive symptoms in individuals who are dependent on alcohol within a short time frame, again highlighting the impact of alcohol on depression . Research has also been conducted with families to try to establish whether a genetic model may explain the co-occurrence of alcohol misuse and depression. The Collaborative Study on the Genetics of Alcoholism (COGA) 39 interviewed 954 alcohol-dependent men and women, their rst degree relatives and a control g
roup. Demographics, medical history and experience of mood and anxiety disorders were assessed for each group and analysed for di erences. The alcohol-dependent group showed higher lifetime rates of mood and anxiety problems than either their relatives or the controls, and for many, these problems were precipitated by a gradual increase in alcohol consumption. Other research has found similar associations in the U, with anxiety and depressive symptoms most common in heavy drinkers (over 50 units a week for men and 35
units a week for women) and heavy drinking more common in those with anxiety and depression 40 . According to the World Health Organisation: “the evidence indicates that a clear and consistent association exists between alcohol dependence and depressive disorders and that chance, confounding variables and other bias can be ruled out with reasonable con dence as factors in this association.” 6 4.4 Personality Disorders Individuals receiving treatment for alcohol-dependence are often also diagnosed with a pe
rsonality disorder 35;72;73 . As well as possibly being a pre-disposing factor to alcohol dependence 74 , a personality disorder can a ect the individual’s use of alcohol in a number of other ways. For example, it may in uence : the clinical course of the alcohol-dependence 75 their response to treatment 76 their risk of relapse 77 Alternatively, alcohol misuse itself may give rise to behaviour that is “labelled” as personality disorder 78 looked at two populations of alcoholics; one being treated
in a short-term hospital treatment unit and one in a six-week residential programme based on therapeutic principles 78 . In both groups, approximately 25% of individuals had features of at least one personality disorder, with borderline personality disorder (BPD) being most common in females and anti-social disorder (ASPD) being prevalent amongst males. Given that people with ASPD have 2 times the average population risk of experiencing alcohol abuse or dependence 43 , these numbers may be an underestimation of the associ
ation between the two. 4.5 Schizophrenia People with severe and enduring mental illnesses, such as schizophrenia, are at least three times as likely to be alcohol-dependent than others in the general population 43;79 and individuals with alcohol problems are also at increased risk of having schizophrenia 80 . Many of the statistics concerning these co-occurring problems are based on surveys conducted in inner-city populations. One study in the U interviewed key workers of all NHS inpatient, day-patient and outpatient A
dult Mental Health (AMH) and Addictions services in the more rural population of east Dorset. Of those with serious mental illness under the care of AMH services, 2% had problems with alcohol, compared to over 40% of those using the Addictions service. However, only half of those with co-occurring disorders in either group recognised the dual nature of their illness and this has implications for their care and the treatment of their needs. • • • The Association between alcohol use and speci c mental hea
lth problems 25 CHEERS? Conclusion It is clear that drinking more than recommended daily limits of alcohol presents risks for many in the general population. Although in the short-term it may provide people with a relatively easy coping strategy for underlying mental health issues such as stress, depression or anxiety, the research suggests that long-term alcohol misuse is damaging. Not only may it serve to worsen the very symptoms it is being used to dampen, but it is associated with a range of other mental health conse
quences. These include depression, anxiety, suicide, risk-taking behaviours, personality disorders and schizophrenia. In addition, alcohol misuse is associated with increased levels of stress, relational con ict and physical injury, which in themselves can contribute to poor mental health. The research also underlines the increased vulnerability faced by individuals as services try to cope with an array of multiple and inter-related issues. It clearly points to the increased level of need encountered by individuals wi
th both mental health and alcohol problems and these may not be the only problems they face. Research shows that risk factors associated with having both a mental health and an alcohol related problem , include: homelessness poverty a history of violence or o endingmore than one period of detention under the Mental Health Act ( failure to respond to mental health services and treatment. Before examining the implications of the research for treatment, policy and practice, recent trends in alcohol consumption and the Gov
ernment’s response to those trends are explored. • • • • • The Association between alcohol use and speci c mental health problems 26 CHEERS? Louise, eacher, 27 ouise began drinking to excess whilst at University with peers but a year after leaving found herself drinking before work and regularly collapsing at the station after work, as she was drinking vodka in the toilets. This occasionally led to arrests for being drunk and disorderly. “I drank a lot at University, but so did eve
ryone. It was seen as fun. There were mishaps but there would always be someone who had done something worse so there was no real re ection on any of it. In hindsight, my drinking changed in the last year of University. Just before my nal year I ended a three year relationship with someone who had become violent, had an abortion, my grandfather died and I was really let down by a close friend. I was clearly depressed. I found that I was breaking down in tears after a heavy night drinking and people were avoidi
ng me. I had no idea why this was happening and never questioned it.” After University, a relationship ended badly and she had to move to her parents’ home. She felt alienated after four years of being surrounded by lots of people. It was at this time she began drinking alone in her room in the evenings. This led to an incident where she turned up to work still intoxicated after a heavy session and was red, leaving her deeply shocked and ashamed. ‘’From this point my drinking rapidly spiralled o
ut of control for the next year-and-a-half. I hurt my family deeply and had no friends. It was like it had taken me over, I felt dead inside and terri ed about what was happening to me.” Finally, after a period she describes as ‘’hell’’ she gave up drinking. ‘’I went to visit a rehab place and it scared me so much I just decided to stop, I nished my postgraduate quali cation in a short time period, began temp work and within a matter of months, I had passed my course, res
tored relationships with my family and got a well paid job.”” She did see a cognitive therapist which was helpful. ‘’She gave me some positive reinforcement, encouraged me to buy my own house and have goals, which is what I needed.’’ But ouise says the drinking and the feelings behind it were never really discussed. It was the break up of a relationship that led her to re-examine her drinking. ‘’At the end of that I had such low self-esteem, guilt and pain that I found myself dri
nking a lot again at home.” Although it was really nothing like before, she decided to do something quickly and attended AA meetings.ouise felt that AA increased her feelings of depression, acknowledging whilst it was helpful to meet people who understood, she found the philosophy very negative. ‘’I found it hard to accept that I was powerless, that I would have to attend meetings every day for the rest of my life, I could not nd a higher power and felt like a failure and found I learnt nothing about m
yself and reasons for drinking.”ouise has got a psychotherapist. She has learned a lot about her mental health, perfectionism, relationships and depression and believes that in slowly changing these patterns she nally understands herself. “While I think I may have a genetic predisposition to alcohol addiction, I don’t think that’s the whole story, my alcohol problems have de nitely been a re ection of my emotional state.’’ The Association between alcohol use and speci c me