
Date Rev iewed March 202 2 1 Th do es not establish a standard of care to be followed in every case It is recognized that each case is different and those individuals involved in providing hea ID: 955830
Download Pdf The PPT/PDF document "is care process model" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Date Rev iewed : March 202 2 1 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Gastric Sleeve Enhanced Recovery after Surgery (ERAS) : Care Process Model Synopsis Algorithm(s) : Date Rev iewed : March 202 2 2 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Date Rev iewed : March 202 2 3 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each ca
se is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Date Rev iewed : March 202 2 4 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Date Rev iewed : March 202 2 5 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist
and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Objective s The objectives of the gastric sleeve ERAS program are to promote overall healing from surgery, decrease opioid pain medicine use an d side effects by using regional anesthesia, advance diet faster and speed up return of bowel function , and decrease length of hospitalization. Background Weight loss surgery in the obese population has been commonplace for many years. Studies have shown reversal or reduction in severity of obesity related medical outcomes. However, this is a relatively new concept in the pediatric population, and a growing problem due to the earlier onset and increasing prevalence of pediatric obesity ( Gur n ani et al., 2015) . Obesity is a systemic disease and poses a challenge to the anesthesiologist and surgeon (Brenn, 2005) . Frequent comorbidities include insulin resistanc e, hypertension, hyperlipidemia, GERD, as well as obstructive sleep apnea. Patients may be on weight loss medications that are of concern to the anesthesiologist, particularly sympathomimetic medications (phentermine) and antihypertensive medications ( i.e. , ACE inhibitors) ( Stephens et al., 2005; Hollmann et al., 2018) . Obesity also creates additional concern for position injuries, which are more common than patients with a normal BMI ( Warner et al, 1994) . The surgical exposure involves steep Reverse Trende lenburg and rotation. These patients must be secu
red to the table to avoid rare but serious injuries from falling or pressure point injuries. The airway is also an area of concern as these patients may be difficult to mask ventilate or to intubate . Patients may have sleep studies, but frequently do not. In general , the surgical time for a sleeve gastrectomy is 1.5 - 2.5 hours. Postoperatively, p atients are typically admitted for a few days, and a main goal of this ERAS protocol is to decrease the to tal length of stay . P ostoperative nausea and vomiting, pain control, and PO intake are some of the challenges during the inpatient portion of the hospital stay. The age range is usually 14 - 18 years but may be trending to include younger patients in the fut ure as efficacy is demonstrated. Core Principles of ERAS (Melnyk et al., 2011) • Preoperative education of patients and family with an introduction to ERAS • Reduced pre - operative fasting, with clear liquid oral carbohydrate loading until 2 hours prior to surgery • Goal - directed strict intraoperative intravenous fluid therapy guidelines to avoid hypo - or hypervolemia • Avoidance of pre - operative mechanical bowel preparation • Avoidance of routine nasogastric tube use • Minimizing long - acting opioid analgesia, in fav or of regional anesthesia with epidural and/or local anesthesia for intra - operative and postoperative pain control when appropriate and using alternative non - opioid medications when appropriate (e.g., non - steroidal anti - inflammatories or acetaminophen) • Ear ly pos
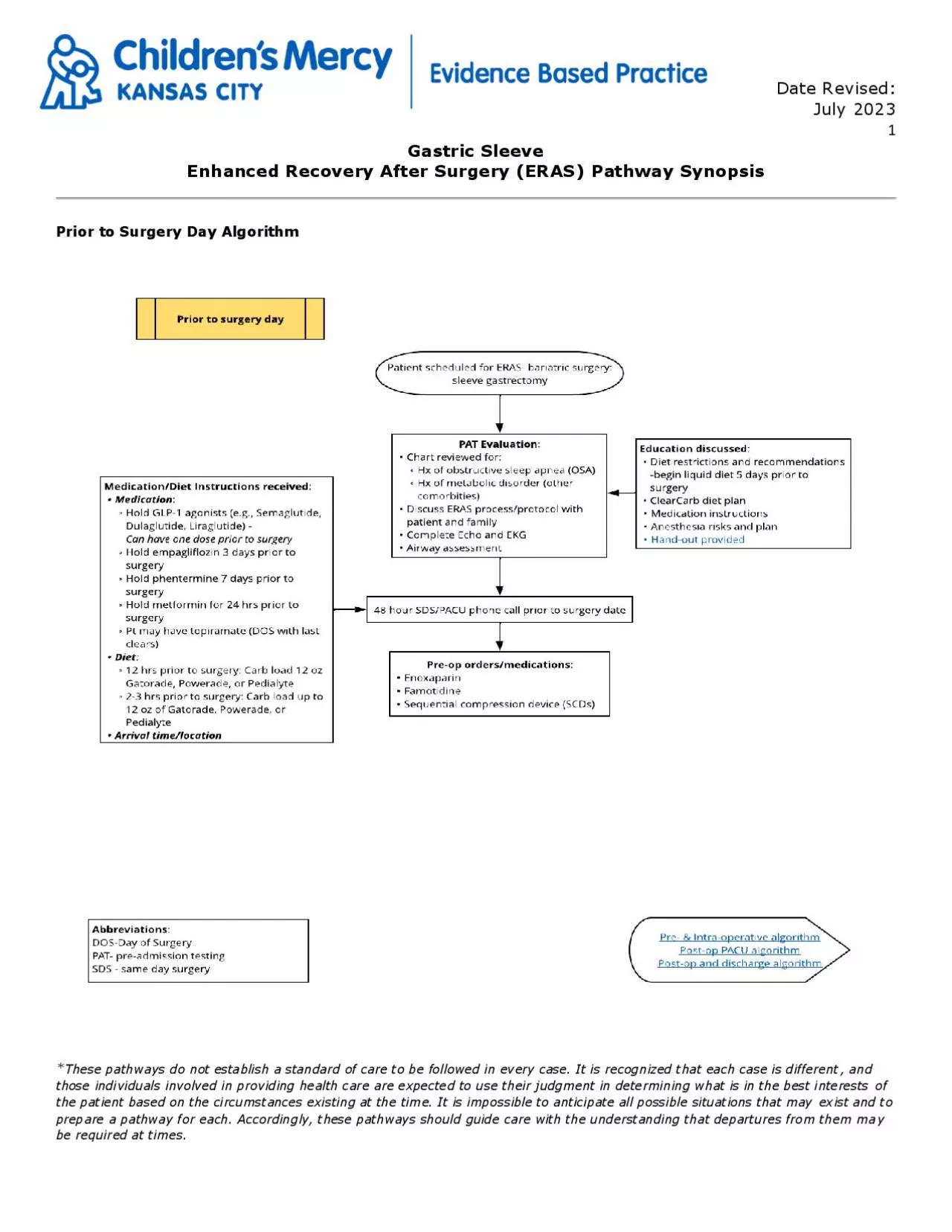
t - operative mobilization • Early post - operative enteral feeding Target Users • Anesthesiologists • Bariatric surgeons • Pre - Anesthesia testing nurse • Post Anesthesia Care nurses • Inpatient floor nurses ERAS Management Recommendations Pre - operative Car e o The concept of ERAS is presented to the patient/family at the initial surgical appointment, and then reinforced during the pre - anesthesia testing (PAT) clinic visit. o At PAT there are educational items discussed including pre - op diet restrictions, medication management , and the risk s of anesthesia. Also discussed some of the core concepts of ERAS, including the emphasis early post - op PO intake and a multimodal pain mana gement approach. Expectation management is crucial in the preoperative phase. o A handout , reviewed by the Health Literacy Committee , is given to the family prior to departing PAT ( A ppendix A ) . Date Rev iewed : March 202 2 6 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may
be required at times. o These patients begin a liquid diet 5 days prior to the scheduled procedure and are contacted 48 hours prior to the procedu re to review arrival time and answer any questions . o On the morning of surgery, the patient drink s carbohydrate rich liquids up to two hours before surgery start time and is administered a scopolamine patch and enoxaparin in pre - op holding . Intra - operative Care The principal goals during the intraoperative care of these patients are : o Safely secure the airway after an IV induction , as these patients may be difficult to bag - mask ventilate or have a difficult airway o Maintain normothermia during the entire procedure o Ensure that antibiotics are administered prior to surgical incision o Minimize the use of long - actin g narcotics o Multimodal pain management including IV acetaminophen and ketorolac o Post - operative nausea and vomiting prophylaxis with dexamethasone and ondansetron o Maintain euvolemia with an emphasis on not administer ing excess IV fluids o Awake extubation while avoiding suctioning of stomach o A conditional recommendation is made for the use of TAP blocks in laparoscopic gastric bypass surgeries, based on the GRADE Evidence to Decision instrument a, and the Summary of Findings Table c . The overall ce rtainty in the evidence is moderate a for use of TAP blocks for reduction of postoperative opioid need and consumption. However, subjective data collected on patients’ pain level using a visual analogu
e scale (VAS) showed the evidence is of moderate to very low evidence a for pain level reduction at zero hours and 24 hours postoperative . Use of TAP blocks for gastric sleeve surgeries at Children’s Mercy will be determined with additional data collected . Post - operative Care The principal goals during the post operative care of these patients are: o Prevent/treat post - operative nausea and vomiting o Multimodal pain control with long - acting opioids as last option o Move towards PO intake as early as possible o Early mobilization o Transit ion from clears to high protein liquids o Focus on early discharge from hospital with home instructions (A pp end ix B). o Clinic follow - up 2 weeks after discharge o General Surgery Post Op Bar iatric power plan (Appendix C). o Bariatric Diet Guidelines associated with General Surgery Post Op Bariatric p ower p lan (Appendix D). Care Questions Answered • Keto rolac in gastric bypass patients and r isk of bleeding • Use of Transverse Abdominal Plane (TAP) blocks and reduction of pain in lap gastric bypass patients Metrics to be Collected Pre - Op Intra - Op Post - Op Scopolamine Patch Dexamethasone /Ondansetron Length of Stay Enoxaparin Euvolemia Time to Ambulation A ntibiotics administered prior to incision Time to Bariatric 2 Diet IV Acetaminophen /IV Ketorolac Long - Acting Opioids Long - Acting Opioids Normothermia Date Rev iewed : March 202 2 7 *Th is care process model do
es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Committee Members and Representation • Jason Fraser, MD , FACS, FAAP | Department of Pediatric Surgery | Committee Co - Chair • Christian Taylor, MD | Department of Anesthesiology | Committee Co - Chair • Azita Roberson , MSN, RN, CPN, APRN, FNP - C | Department of Anesthesiology | Committee Member • Stephanie Crandon, BSN, RN, CPN | Quality Improvement Program Coordinator 4 West| Committee Member • Stephanie Otis, MSN, RN, CPEN | Surgery | Committee Member • Michelle Be i sly, MSN, RN, CPN | Education Coordinator II 4 West | Committee Member EBP Department Members • Todd Glenski, MD, MSHA, FASA |Department of Evidence Based Practice & Department of Anesthesiology • Andrea Melanson, OTD, OTR/L | Department of Evidence Based Practice Approval Process Department/Unit Date Approved 4 West: Post - Operation Unit October 2021 Anesthesiology October 2021 Evidence Based Practice October 2021 Bariatric Surgery October 2021 S
ame Day Surgery/Post - Anesthesia Care Unit October 2021 Version History Date Comments Oct ober 20 21 First version March 2022 Second version; updated formatting and hyperlinks Planned Revisit Da te September 15, 2022 Date Rev iewed : March 202 2 8 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. References Brenn B. R. (2005). Anesthesia for pediatric obesity. Anesthesiology C linics of North America , 23 (4), 745 – x. https://doi.org/10.1016/j.atc.2005.08.008 Hollmann, C., Fernandes, N. L., & Biccard, B. M. (2018). A s ystematic r eview of o utcomes a ssociated w ith w ithholding or c ontinuing a ngiotensin - c onverting e nzyme i nhibitors and a ngiotensin r eceptor b lockers b efore n oncardiac s urgery. Anesthesia and A nalgesia , 127 (3), 678 – 687. https://doi.org/10.1213/ANE.0000000000002837 Gurnani, M., Birken, C., & Hamilton, J. (2015). Childhood o besity: c auses, c onsequences, and m anagement. Pediatric
C linics of North America , 62 (4), 821 – 840. https://doi.org/10.1016/j.pcl.2015.04.001 Melnyk, M., Casey, R. G., Black, P., & Koupparis, A. J. (2011). Enhanced recovery after surgery (ERAS) protocols: t ime to change practice? Canadian Urological Association J ournal = J ournal de l'Association des urologues du Canada , 5 (5), 342 – 348. https://doi.org/10.5489/cuaj.11002 Stephens, L. C., & Katz, S. G. (2005). Phentermine and anaesthesia. Anaesthesia and I ntensive C are , 33 (4), 525 – 527. https://doi.org/10.1177/0310057X05033004 18 Warner, M. A., Warner, M. E., & Martin, J. T. (1994). Ulnar neuropathy. Incidence, outcome, and risk factors in sedated or anesthetized patients. Anesthesiology , 81 (6), 1332 – 1340. Date Rev iewed : March 202 2 9 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. A ppendix A Gastric Sleeve ERAS Pre - op Protocol Date Rev iewed : March 202 2 10 *Th is care process model do es not establish a standard of care to be followed in every
case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. A ppendix B Gastric Sleeve Discharge Instructions Date Rev iewed : March 202 2 11 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Date Rev iewed : March 202 2 12 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the
time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Appendix C General Surgery Post Op Bariatric Power Plan Date Rev iewed : March 202 2 13 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. Appendix D Bariatric Diet Guidelines How to order: • Bariatric Diet 1: Water • Bariatric Diet 2: Clear Liquids • Bariatric Diet 3: High Protein Full Liquids • Bariatric Diet 4: High Protein Soft Foods Diet Description: • Bariatric Diet 1: Water (First phase of the diet for post - bariatric sleeve gastrectomy) Administer 1 - ounce per hour of room temperature water as t olerated. This diet usually lasts 12 - 24 hours before proceeding to Bariatric Diet 2. However, if patient is tolerating 1 - ounce per hour, he/she may advance to Bariatric Diet 2 in as little as 3 - 4 hours
. Please call provider to advance to next stage. o Speci al instructions: Start immediately postoperatively, only water, no carbonation, no caffeine, no straws. Patient should sip slowly and stop when full. • Bariatric Diet 2: Clear Liquids (Second phase of the diet for post - bariatric sleeve gastrectomy patients ) Administer 2 - 4 ounces/hour, given in 1 - ounce increments. Patient needs to take 64 - 96 ounces successfully, before discharge home. Patient may then proceed to Diet 3, protein shakes, before discharge, if they prefer; however, this is not required for disc harge. Please call provider to advance to Bariatric Diet 3. o Special instructions: Only sugar free clear liquids, no carbonation, no caffeine, no straws. Patient should sip slowly and stop when full. • Bariatric Diet 3: High Protein Full Liquids (Third phase of the diet for post - bariatric sleeve gastrectomy) 24 - 32 ounces of high protein liquids (such as Premier Protein) total, given in 4 - ounce protein drink “meals”, 5 - 6 times a day and 4 - 8 ounces of clear liquids between meals, given over an hou r. Dehydration is the most common complication in the first 3 weeks after surgery, so the clear liquids are more important to push than the protein drinks. o Special instructions: No carbonation, only sugar free liquids or water for clears, no caffeine, no s traws • Bariatric Diet 4: High Protein Soft Foods (Fourth phase of the diet for post - bariatric sleeve gastrectomy) Goal of 60 - 90 grams of protein per day AND 64 fluid ounces water or sugar fre
e clear liquids (8 cups per day minimum) AND 24 - 32 fluid ounces of high protein liquids (these will count towards total protein/day). o Special instructions: Provide patient 4 - 6 meals per day, every 2 - 3 hours, including: soft, moist, diced or ground protein foods; 2 - 4 tablespoons of soft, moist fruit or vegetables . Each meal should be 30 minutes. No carbonation, no caffeine, no straws. Adequacy: • Nutrient analysis of the menus is available from Webtrition and reflects available nutrient information. Webtrition pulls nutrient information from either the USDA Standard Reference database (which includes 36 of the 41 RDA/DRI nutrients) or the manufacturer’s information (manufacturers are required only to provide 13 of the 41 RDA/DRI nutrients). Because of this, nut ritional analysis data may be incomplete for some foods and /or some nutrients that are listed in the DRI. • Due to the therapeutic restrictive nature of this diet, some nutrients do not meet 100% of the DRI’s. • Ongoing outpatient nutrition monitoring is required. *Complete analysis on pages 2 - 3 Guidelines: • The day of surgery is counted as day 0 Date Rev iewed : March 202 2 14 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anti
cipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. House Diets: • House diets are available for inpatients with orders for Bariatric Diet 2 - 4. Refer to the Diet M anual found on Scope for daily menu options. * Date Rev iewed : March 202 2 15 *Th is care process model do es not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the pat ient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare care process models for each. Accordingly, th is care process model should guide care with the understanding that depa rtures from them may be required at times. 1Pratt, Janey S.a., et al. “ASMBS Pediatric Metabolic and Bariatric Surgery Guidelines, 2018.” Surgery for Obesity and Related Diseases , vol. 14, no. 7, 2018, pp. 882 – 901., doi:10.1016/j.soard.2018.03.019e 2 Editors: Weight Management Dietetic Practice Group; Sue Cummings, MS, RD, LDN, and Kellene A. Isom, MS, RD, LDN. (2015). A.N.D Guide to Bariatric Surgery (2nd edition). NP: Academy of Nutrition and Dietetics. Reviewed: 07/30/20 by Lora Edwards, RD; Kate Barkman, RD Approved by Dr. Fraser, MD; Denice Wehausen - Mo