
Thisguideline shouldnotbeused forthefollowing InfecteddiabeticulcerorvascularulcerHumanoranimalbiteCriticalillness ClinicalconcernfornecrotizingfasciitisPeriorbitalororbitalcellulitisBacteremi ID: 939592
Download Pdf The PPT/PDF document "ANMCGuidelineforUncomplicatedSkinandSoft..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

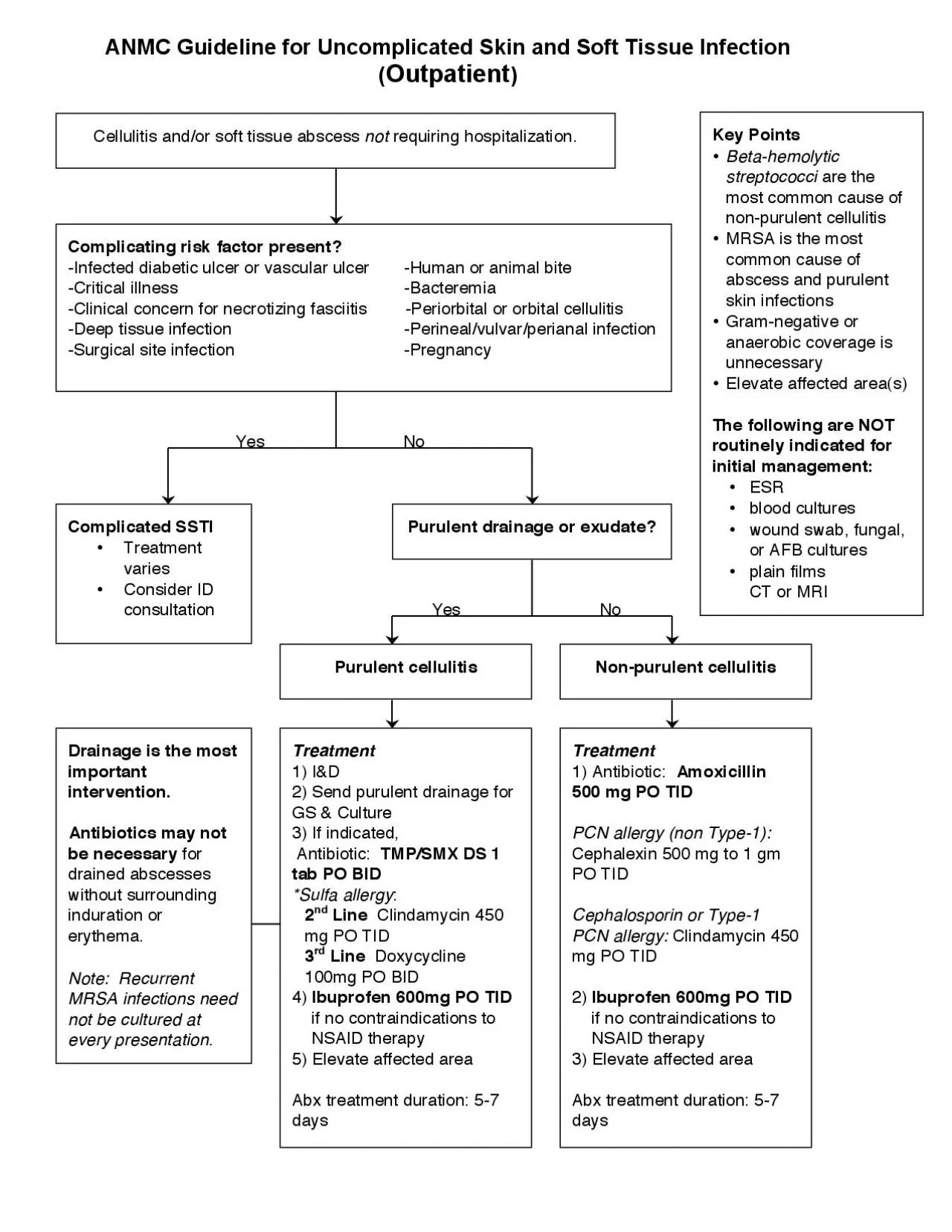
ANMCGuidelineforUncomplicatedSkinandSoftTissueInfection Thisguideline shouldnotbeused forthefollowing: - Infecteddiabeticulcerorvascularulcer-Humanoranimalbite-Criticalillness -Clinicalconcernfornecrotizingfasciitis-Periorbitalororbitalcellulitis-Bacteremia -Surgicalsiteinfection-Pregnancy Complicatingriskfactorswarrantalternativetreatmentstrategies;considerInfectiousDiseasesconsultation KeyPoints: Beta-hemolyticstreptococciarethemostcommoncauseofnon-purulentcellulitis MRSAisthemostcommoncauseofabscessandpurulentskininfections Gram-negativeoranaerobiccoverageisunnecessary Elevateaffectedarea ThefollowingareNOTroutinelyindicated forinitialmanagement : ESR bloodcultures woundswab,fungal,orAFBcultures plainfilms CTorMRI Outpatient SuspectedPathogen(s) RecommendedTreatment OtherComments Cellulitis without purulentfocus Betahemolytic Streptococci (MostcommonlyGrpA,also GrpB,GrpC,GrpGstrep) 1) Antibiotic: Amoxicillin500mgPOTID Alternative1 st lineorPCNallergy: Cephalexin500mg-1gmPOTID CephalosporinorType-1PCNallergy: Clindamycin450mgPOTID 2) Ibuprofen600mgPOTID ifno contraindicationstoNSAIDtherapy 3)Elevateaffectedarea AbxTreatmentDuration: 5-7days Cellulitis with purulentfocus Beta - hemolytic Streptococci MethicilinSusceptible Staphylococcusaureus (MSSA) MethicilinResistant Staphylococcusaureus (MRSA) 1)I&D 2)SendpurulentdrainageforGS&Culture 3)Ifindicated, Antibiotic : TMP/SMXDS1tabPOBID *Sulfaallergy : 2n
dLine Clindamycin450mgPOTID 3rdLine Doxycycline100mgPOBID 4) Ibuprofen600mgPOTID ifno contraindicationstoNSAIDtherapy 5) Elevateaffectedarea Drainageisthemostimportantintervention. Antibioticsmaynotbenecessary fordrained abscesseswithoutsurroundingindurationor erythema AbxTreatmentDuration: 5-7days Note:RecurrentMRSAinfectionsneednotbe culturedateverypresentation ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! e y Points Beta-hemolytic streptococci are the most c o mm o n ca u s e o f n o n-p u r u l e nt c e llulitis M R S A is th e m o st c o mm o n cause of abscess and purulent skin infections G ram-n e gativ e o r ana e r o bic c o v e rag e is unnecessary Elevate affected area(s) Th e following ar e NOT routin e ly indicat e d for initial manag e m e nt: E S R bl oo d c u lt u r e s wound swab, fungal, or AFB cultures plain films, CT or MRI 2-3 days? o tic S t e p-d o wn Th e rapy: Cephalexin 1gm PO TID *Cephalosporin or Ty pe-1 PCN allergy: Clindamycin 450 mg PO TID e lin e for Uncomplicat e d Skin and Soft Tissu e Inf e ction (Inpati e nt) e s e nt? e ct e d diab e tic u lc e r o r vasc u lar u lc e r - Hu man or animal bite o nc e rn f o r n e cr o tizing f a sciitis, calc u lat e L R I N EC score and obtain immediate surgical consultation. Dee p tiss ue inf e cti o n
-P e rin e al/v u lvar/p e rianal infection o e ous absc e ss pr e s e nt? e rf o rm b e dsid e u ltras ou nd and/ o r n ee dl e aspiration if uncertain) e d SSTI Treatment varies Consider ID consultation e s o e ous absc e ss o Blood cultures if systemically ill, S u perficial wo u nd c u lt u re N OT e nt drainag e or e xudate Plain film only if concern for foreign o dy Co nsid e r u ndrain e d f o c u s o f infection o For non-purulent cellulitis, consider IV vancomycin Co ns u lt I D services e s e nt c e llulitis o tic S t e p-d o wn Th e rapy: o e s 5 days sufficient for well-drained abscess e nt c e llulitis ou t s u rr ou nding c e llulitis Du rati o n o f th e rapy may b e e xt e nd e d f o r 1) I&D 2) S e nd p u r u l e nt drainag e f o r G S & Cu lt u re 3) Antibiotic: Vancomycin 1 gm IV q12hr 4) Ibuprofen 600mg PO TID if no c o ntraindicati o ns t o N S AI D therapy 5) El e vat e aff e ct e d ar e a Blood cultures if systemically ill, diabetic, or other immunosuppression S u perficial wo u nd c u lt u re N OT indicated Plain film only if concern for foreign b o dy 1) Antibiotic: Cefazolin 2 gm IV q8hr *Cephalosporin or Type-1 PCN allergy: Clindamycin 600 mg IV q8hr 2) Ibuprofen 600mg PO TID if no c o ntraindicati o ns t o N S AI D therapy 3) El e vat e aff e ct e d ar e a 4) Treat tinea pedis if applicab