
Outline Tooth development phases Preeruptive period Period of eruption of the primary dentition Static period of the primary dentition Tooth Development Phases 1 Initiation The process of tooth development starts as early as 7 weeks in ID: 574137
Download Presentation The PPT/PDF document "Chronology and morphology of primary and..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.





Slide1
Chronology and morphology of primary and permanent teeth Slide2
Outline
Tooth development phases
Pre-eruptive period
Period of eruption of the primary dentition
Static period of the primary dentitionSlide3
Tooth Development Phases
1- Initiation
The process of tooth development starts as early as 7 weeks in
utero
In this phase, the locations of teeth are established with the appearance of tooth germs
.Slide4
Tooth Development Phases
2- Morphogenesis
The shape of the teeth is determined in this phase.Slide5
Tooth Development Phases
3-
Histogenesis
Differentiation of cells takes place to produce the fully formed dental tissues.Slide6Slide7
The primary epithelial bands divides into:
Vestibular lamina
(
buccally
).
Dental lamina
(
lingually
).
The dental lamina contributes to the formation of the teeth.
Underlying
MesenchymeSlide8
Tooth germ formation
Bud stage: (initiation)
The enamel organ appears as a simple ovoid epithelial
mass
Surrounded
by
mesenchyme
.
Mesenchyme
separated from the epithelium by a basement membrane.Slide9
Tooth germ formation
Cap stage (morphogenesis)
Invagination
of the deeper surface of the enamel organ.
Peripheral cells start to be arranged as
external and internal enamel epithelium
.Slide10
Cap stage Slide11
Tooth germ formation
Bell stage
The shape of the internal enamel epithelium decides the shape of the crown.Slide12
Bell stage Slide13
Bell stage
Cells of the inner enamel epithelium differentiate into
Ameloblasts
Adjacent cells from the dental papilla will differentiate into
Odontoblasts
Odontoblasts
produce pre-dentine and dentine.
The presence of dentine induces
Ameloblasts
to form enamel
Apposition of enamel and dentin will be followed by calcificationSlide14
Calcification
Starts between 14 and 16 weeks of intrauterine life for primary teeth
Begins in cusp tips and
incisal
edges of teeth and continues
cervically
Very sensitive process that takes place over a long period of time.Slide15
Calcification
Any severe systemic event during the development of teeth will result in some dental abnormality
Chronological enamel defects.Slide16
Calcification
Different teeth will show defects at different levels of the crown depending on the stage of crown formation.Slide17
Eruption
Eruption
is the movement of teeth within and through the bone of the jaws and the overlying mucosa to appear in the oral cavity and contact the opposing teeth.
Emergence of the tooth is the first sign of appearance in the oral cavity.Slide18
Pre-eruptive phase
: period during which the tooth root begins its formation and begins to move towards the surface of the oral cavity from its bony vault.Slide19
Eruptive phase (
prefunctional
):
period of gingival emergence until contact is achieved with the opposing tooth.
Functional eruptive phase:
after the tooth meets its antagonist. A dynamic unit throughout life. Slide20
Factors influencing tooth formation and eruption
Why is it difficult to study and understand the process of eruption?
T
ooth
structure and eruption vary from one species to another
Histological studies in humans are rarely possible because of the inaccessibility of tissue for sampling and ethical considerationsSlide21
Theories of eruption
1- Root formation
2- Hydrostatic pressure
3- Bone remodeling
4- Periodontal ligament Slide22
Root formation theory
The space for the growing root is accommodated by
occlusal
movement of the tooth crown
However;
Some teeth with extensive root development fail to erupt
A study using dogs, showed that the tooth itself played no part in the eruptive processSlide23
Hydrostatic pressure theory
Studies using dogs demonstrated that the tissue pressure apical to the erupting tooth was greater than
occlusally
, theoretically generating an eruptive force
However;
The study only compared pressure differentials but whether this pressure difference actually caused eruption is not proven Slide24
Bone remodeling theory
Bone remodeling around the tooth causes eruption
However;
Animal studies showed that bony remodeling occurs
around the dental follicle regardless
of the presence of a
toothSlide25
Periodontal ligament theory
Strong evidence exists to show that the periodontal ligament, which is derived from the dental follicle, provides the force required for eruption mainly by fibroblast contraction
However;
in vitro
tissue studies have limitations
Slide26
In conclusion
There is no evidence that one hypothesis fully explains tooth eruption, and that eruption is likely to be a
multifactorial
processSlide27
Basic biology of tooth eruption
1- Bone
resorption
Resorption
appears to be genetically controlled and
not mechanically
by the eruption of the
tooth
2- Role of the dental follicle
Removing
the follicle means the tooth will not erupt
while
leaving it and replacing the tooth with an artificial replica
means the tooth will erupt3- Cellular events and molecules
Certain molecules will recruit mononuclear cells into the dental follicle Slide28
Control of eruption
1- Hormonal control
2- Systemic conditions
3-
Physical
control mechanismSlide29
Hormonal control
Most eruption occurred in the late evening indicating that eruption was probably under hormonal control
Mainly due to the effects of the late evening secretion of
growth hormone and thyroid hormone.
Children with growth hormone deficiency had delayed tooth eruptionSlide30
Systemic conditions
Nutritional deficiency (extremes)
Preterm and low birth weight infants
Cerebral palsy
Anemia
Renal failure
Genetic disorders
Apert
syndrome
Cleidocranial
dysostosis
Down syndrome
Ectodermal
dysplasia
Gardner syndrome
OsteopetrosisSlide31
Physical control mechanism
According to the equilibrium theory teeth remained in a position within the jaws where forces acting in equal and opposite directions cancelled each other
Oral musculature, soft tissue pressures,
masticatory
forces, and eruptive force.Slide32
Pre-eruptive period
Upper anterior gum pad (
intercanine
width) is typically wider than the lower anterior gum pad
Upper anterior gum pad protrudes (
Overjet
) about 5mm
Overbite about 0.5mm.Slide33
Pre-eruptive period
Marked palatal width increase and a decrease in the
overjet
over the first 6 months of postnatal life.Slide34
Pre-eruptive period
Labial
frenum
is usually hypertrophic but it does not hinder suckling
Retro incisal papilla is hypertrophic.Slide35
Pre-eruptive period
Palate is straight at birth. Becomes concave under the effect of growth of the alveolar bone
Tongue is relatively large.Slide36
Oral mucosa
Epstein pearls.
Bohn nodules
Dental lamina cyst.Slide37
Epstein pearls
Small white or greyish white lesions
Present in about 80% of neonates.
Formed along the
midpalatine
raphe.Slide38
Epstein pearls
Considered remnants of epithelial tissue trapped along the raphe as the fetus grows.
Disappear within a few weeks of life.Slide39
Bohn nodules
Formed along the buccal and lingual aspects of the dental ridge and on the palate away from the raphe.Slide40
Bohn nodules
Considered remnants of mucous gland tissue and are histologically different from Epstein pearls.
Disappear spontaneously in the early months of life.Slide41
Dental lamina cysts
Found on the crest of the maxillary and mandibular dental ridges.
Are remnants of the dental lamina.
Slough within the first few months of life.Slide42
Dental lamina cysts
Differential diagnosis: natal teeth.
No treatment necessary.Slide43
Period of eruption of the primary dentition
Commences at 6 months and is well established by 30-36 months
Maximum growth of the jaws occurs during this period.Slide44
Deciduous Teeth
20 in number, 10 in each jaw.
There are no premolars in the deciduous dentition.
The primary molars are replaced by the permanent premolars.
The permanent molars erupt distal to the primary second molars.Slide45
Nomenclature
Beginning with the midline, the teeth are named as follows:
Central incisor.
Lateral incisor.
Canine.
First molar.
Second molar.Slide46
Tooth numbering
Palmer Notation Method
.
Children’s 20 primary teeth are lettered “A” through "E" in each quadrant.
Universal Numbering System.
FDI Two-Digit Notation
.
The currently accepted convention to view the FDI notation chart is from the perspective of the
patient's right
.Slide47
FDI Two-Digit Notation
1s are central incisors, 2s are laterals, 3s are canines, 4s are 1st premolars etc., up through 8s which are 3rd molars
The
permanent teeth
quadrants are designated 1 to 4 such that 1 is upper right, 2 is upper left, 3 is lower left and 4 is lower right
In the
deciduous dentition
the numbering is correspondingly similar except that the quadrants are designated 5,6,7 and 8. Slide48
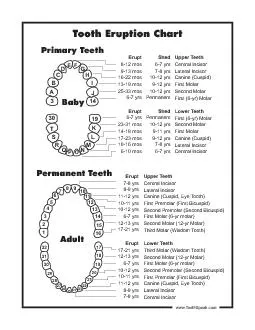
Chronology of eruption of primary teeth
1
st
tooth at approximately 6 months
Usually the lower central incisorSlide49
Chronology of eruption of primary teeth
All eruption schedules are
estimates
No two individuals are alike
.
Multiple parameters: race, gender, ethnicity, familial environment, heredity.Slide50
Chronology of eruption of primary teeth
Maxillary
Mandibular
Central incisors
6-10 months
5-8 months
Lateral incisors
8-12 months
7-10 months
Canines
16-20 months
16-20 months
First molars
11-18 months
11-18 months
Second molars
20-30 months
20-30 monthsSlide51
Sequence of eruption
A then B then D then C then E
Mandibular
precede maxillary most of the time.Slide52
Rhythm of eruption of primary teeth
Symmetrical groups of 4 teeth every 6 months
Teeth erupt symmetrically in both jaws, simultaneously and in pairs.Slide53
The ‘six/four’ rule for primary tooth emergence
Four teeth emerge for each 6 months of age.
6 months: 4 teeth (lower & upper As)
12 months: 8 teeth (1+upper & lower Bs)
18 months: 12 teeth (2+ upper & lower Ds)
24 months: 16 teeth (3+ upper & lower Cs)
30 months: 20 teeth (4+ upper & lower Es)Slide54
Static period of the primary dentition
Period of stability of the primary teeth
3-6 years of age
Child has 20 primary teeth in their final and functional position
Occlusion is well establishedSlide55
Static period of the primary dentition
Occlusal
features
Occlusion of the primary second molar
Inter-arch relationship of primary teethSlide56
Occlusal
features in the established primary dentition
Incisor teeth tend to be spaced
Primate spaces exist between upper B & C and between lower C and DSlide57
Occlusal
features in the established primary dentition
Upper incisors are upright
Incisor relationship is more towards edge to edge.Slide58
Occlusal
features in the established primary dentition
Long axis of primary teeth is parallel
Absence of the curve of
Spee
In general, teeth in the primary dentition tend to be well aligned.Slide59
Classification of occlusion of the primary second molar
Look at the distal aspect of the primary second molar
Flush terminal plane
Mesial
step
Distal stepSlide60
Flush terminal planeSlide61
Mesial stepSlide62
Distal stepSlide63
Inter-arch relationship of primary teeth
Each tooth occludes with two opposing teeth except for the lower central incisors and the upper second molars.
Canine is a key to occlusion in the primary dentition.
Look at the long axis of the canineSlide64
Canine relationship
Long axis of the canine should be placed in the midline between the lower D and C for a class I relationship.Slide65
Inter-arch relationship
Natural wearing away of the canines is an important physiologic process that facilitates movement of the mandible
In children raised on soft food the natural wearing process may be slowed down
May have to carry out selective grinding on primary canines, especially in the presence of a unilateral
crossbite
.