
Chris Wichman PhD Department of Biostatistics College of Public Health University of Nebraska Medical Center Topic Outline Traditional Research Design Concepts Design Changes to Accommodate Community Based Research ID: 917415
Download Presentation The PPT/PDF document "Biostatistical Design Considerations for..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
Biostatistical Design Considerations for community engaged research
Chris Wichman, PhD
Department of Biostatistics
College of Public Health
University of Nebraska Medical Center
Slide2Topic Outline
Traditional Research Design Concepts
Design Changes to Accommodate Community Based Research
Outcomes and Interpretation
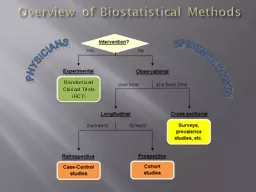
Slide3Traditional Research design concepts
Slide4Definitions
Study / Experimental Unit – smallest unit to which study conditions are independently applied.
Observational Unit – smallest unit on which measurements are taken
Condition / Treatment Design – how are study conditions organized
Study / Experimental Design – how are experimental units organized
Slide5Goal
Utilize a design that:
addresses study intent;
minimizes bias;
addresses appropriate questions about treatments / conditions of interest
Slide6Study intent
Must be tied directly to research question and resulting hypotheses.
Comparative Effectiveness – two-sided hypotheses
Superiority (inferiority) – one-sided hypotheses
Non-inferiority – equivalence tests
Quality Improvement – can use any type of hypothesis, but not required
Feasibility – focus on ability to conduct the study / implement the process
Sustainability – longitudinal – can gains made be maintained
Slide7Condition / treatment designs
Single factor, two or more levels
Multi-factor with main effects
Multi-factor with interactions
Ex. 4 factor levels, interested in mean
of each level
Ex. Factor 1: 2 levels; factor 2: 3 levels
interested in means of factor 1 levels
Without regard to factor 2
and vice versa
Ex. Factor 1: 2 levels; factor 2: 3 levels
interested in the effect of factor 1 &
factor 2, allowing for a different effect
of one factor considering the other.
Slide8Study designs
How the subjects are arranged relative to factor-level combinations.
Researcher specifies the design
Examples:
Completely Randomized
Blocked
Pre – Post
Repeated Measures
Nested Design
Split / Crossover Design
Slide9Minimizing bias
Confounding
Randomization
Blocking
Stratification
Balance
Slide10Confounding variables
Definition 1: “Two variables are confounded if they appear in such a pattern that their separate effects cannot be distinguished”.[Moses, 2009].
Definition 2: – Confounding variables are those that may compete with the exposure of interest (
eg
, treatment) in explaining the outcome of a study”. [Skelly, et al, 2012].
“Confounding factors may mask an actual association or, more commonly, falsely demonstrate an apparent association between the treatment and outcome when no real association between them exists”[Skelly et al, 2012].
Slide11Randomization
Randomly assign study conditions (treatments) to subjects
May need / want to do this by strata to balance confounders
1, 2, 3, 4, 5, 6, 7, 8,9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20
Subjects
1, 2, 3, 5, 7, 9, 10, 12, 15, 19
4, 6, 8,11, 13, 14, 16, 17, 18, 20
Condition 1
Condition 2
Slide12Blocking
…
Block 1
Block B
Block – Groupings of subjects that are alike
Ex. Domestic Violence CBOs – Blocking would be done on service type: crisis, shelter, support group, etc.
Replicate the base study within each block at least once (all conditions present at least once)
Block can be modeled as a factor with B levels
Slide13Stratification & balance
Stratification
Natural groupings in which we want to ensure sufficient representation
When building a sample of participants, want to make sure sex, age, education, race / ethnicity of the target population is represented.
Analytically, subgroup analyses – additional way of dealing with confounders
Balance
“Equal” representation under each study condition
Slide14design changes to accommodate Community based research
Slide15Design Changes
Larger in scale – more than one site
Sites often become the study / experimental unit
Individuals at a given site are units of observation
Site outcomes are an aggregation of measures on OUs.
Slide16Sample size Determining factors
Depends on the statistical hypothesis to be tested, study design, type of primary outcome, number of groups, type of analysis that will be used
Need preliminary/pilot data to estimate effect size, a measure of the expected differences between the groups.
Balance between type I and type II errors
Justice System
- Trial
Innocent
Guilty
Guilty Verdict
Type I Error
Correct
Not Guilty Verdict
Correct
Type II Error
Statistics
– Hypothesis Test
Null True
Null
False
Reject Null
Type I Error
(False positive)
Correct (Power)
Fail to RejectCorrectType II Error(False negative)
𝛼
𝛽
Slide17Power and sample size
Given the effect to be measured, the uncertainty in the measurement, and the allowable type I error rate:
what sample size do I need to achieve 80% power to reject the null hypothesis when the null hypothesis is wrong?
Slide18Sample size analysis
Less straight forward than in traditional studies
Must account for clustering
Process balances number of clusters (EUs) and number of OUs
Requires researchers to have a good understanding of numbers per cluster
Seasonal / time effects (random effect of time)
Cluster type effects
Local issues
Slide19Biggest Issue to Understand
Power cannot be increased by an increase in observational units alone
At some point, you must increase the number of clusters
Example: Dichotomous outcome, 9 clusters available, each cluster can support 320 to 360 observational units. Effect size to be detected is moderately large (0.72)
Slide20Desired Design
9 clusters
320 – 360 subjects per cluster
Dichotomous outcome effect size = 0.72
Minimum power = 0.80
Slide21Optional Design
Use original cluster as a design block
Cluster on “practitioner” w/in block
Average of 4 clusters per block
Average of 80-90 subjects per cluster
Slide22Cluster vs block
Cluster
Blocking
CBO1
CBO9
CBO9
CBO1
Slide23Failing to account for clustering
Unexplained variance is underestimated
Type I error is inflated (false importance)
Possible Simpson’s Paradox Issues
Conclusions change when the clustering is accounted for compared to when it is ignored
Slide24Model Based analyses of clustered studies
Requires mixed models (fixed and random effects)
Accounts for correlation, random time and cluster effects
Interpretation of results are less straight forward
Especially for observational unit level effects
Slide25Typical Outcomes FOR CBR
Slide26Outcome and measurement level
Reach – measured on the cluster level
Effectiveness – measured on the cluster level
Implementation – measured on the cluster level
Improvement – measured on the cluster and / or observational levels
Maintenance – measured on the cluster and / or observational levels
Slide27Reach
Definition of eligible
All comers?
New clients only (naïve to the program)
Previous clients meeting specific criteria
Based on type of interaction (subset of all comers)
Definition for number referred
Need to define a failure
Certain number of encounters before failure
Extenuating Circumstances
Acute / crisis vs normal encounter
Slide28Effectiveness
Definition of participation
Show up once
75% or more
etc
Slide29improvement
At the cluster level – proportion
At the observational level – proportion or numerical
Improvement could be defined as:
% change in a targeted outcome
Difference scores
Specific time point comparison between groups
Slide30maintenance
Utilizes the same outcome measure as improvement
Requires a longitudinal study to address
PI / research team need to define
apriori
what maintenance means (equivalence window)
By hypothesis, this should really be a designed equivalence test
Issue, typically comes about after a comparison period (primary outcome for power)
Solution – use post-hoc (1-2
α
) confidence interval
Want the interval to contain 0
Slide31implementation
Adherence to the Protocol =
Dosing
Automatic reminders
Automatic reminders + small group sessions
Automatic reminders + small group sessions + incentive
Consistency
Do process and / or procedures change based on time, day, or contact type?
Adherence to core principles
Are the expectations of the process / protocol adhered to
Slide32Conclusion
Traditional Study Design Principles carry over to Community Based Research
Study units are typically at least one level above the observational unit
Sample size for clustered trials must strike a balance between number of clusters and number of observational units
Studies are typically designed to get at cluster level outcomes
Observational unit level performance can be captured – just harder to implement and interpret
Slide33Questions?
Slide34references
Moses, LE. Statistical Concepts Fundamental to Investigations. Chapter 1: Medical Uses of Statistics, 3
rd
Ed. Editors:
Bailar
III, JC and
Hoaglin
, DC. Wiley & Sons, Hoboken, NJ 2009.
Skelly AC,
Dettori
JR, Brodt ED. Assessing bias: the importance of considering confounding.
Evid Based Spine Care J
. 2012;3(1):9–12. doi:10.1055/s-0031-1298595