
K G M U Lucknow INTRODUCTION Ball and socket type of synovial joint Multiaxial Range of motion restricted weight bearing BONES Femoral head gt12 of sphere Ball Acetabulum vinegar cup ID: 1044725
Download Presentation The PPT/PDF document "Dr P K Sharma Professor Department of An..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.





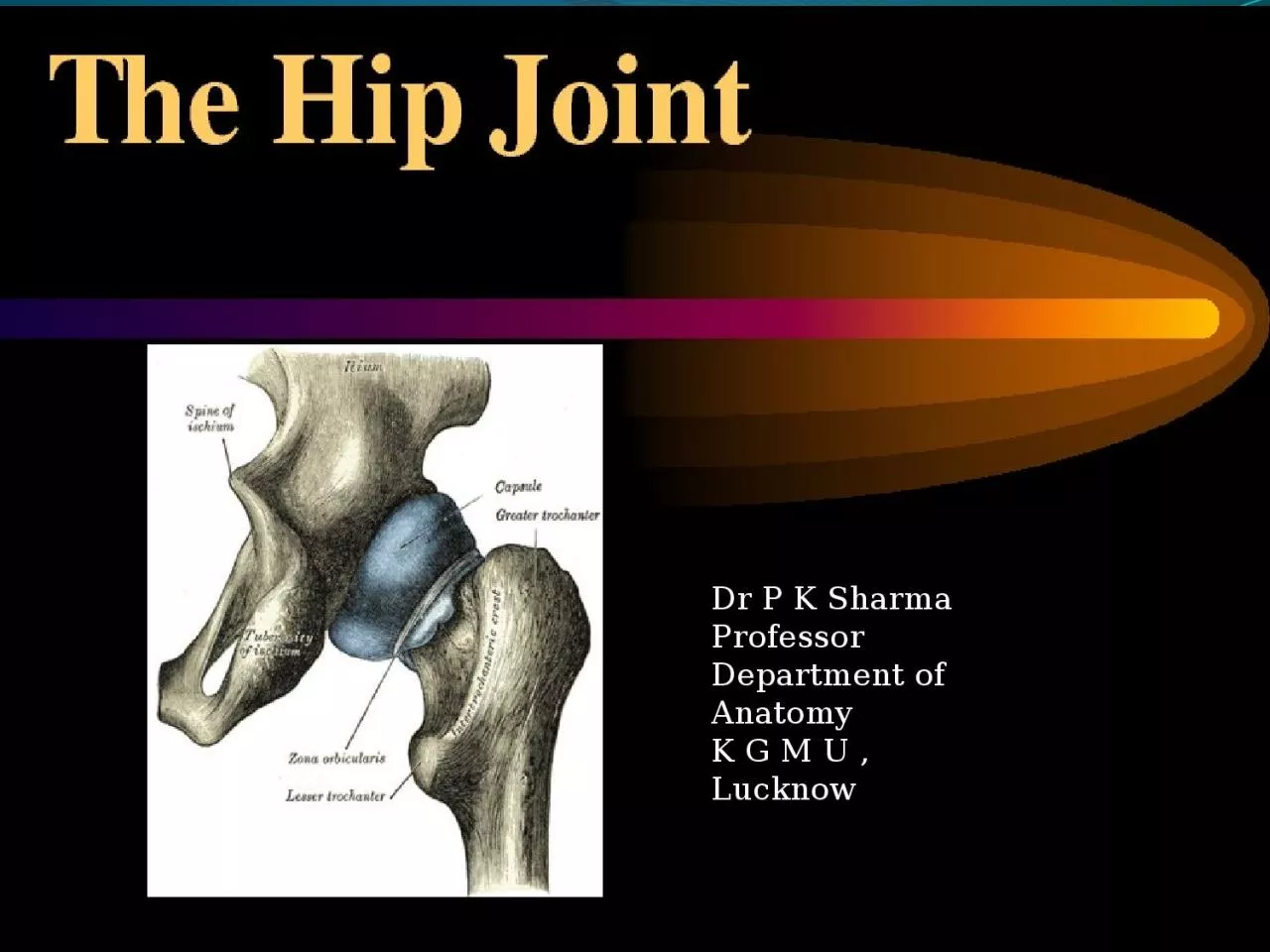
1. Dr P K SharmaProfessorDepartment of AnatomyK G M U , Lucknow
2. INTRODUCTIONBall and socket type of synovial jointMultiaxialRange of motion restricted (weight bearing)
3. BONESFemoral head ->1/2 of sphere-Ball Acetabulum-vinegar cup-Socket Head of the femur articulates with acetabulum
4. ARTICULAR SURFACESHead of Femur- hyaline cartilageNonarticular-fovea capitis Acetabulum-Articular surface -horse shoe shaped hyaline cartilage covered
5. LIGAMENTS OF HIP JOINTCapsular ligament(joint capsule)Ilifemoral ligament-ligament of Bigelow(strongest)Pubofemoral ligamentIschiofemoral ligamentTransverse acetabular ligamentAcetabular labrumLigamentum teres femoris.
6. CAPSULAR LIGAMENTStrong dense fibrous sacInner fibres circular, outer fibres longitudnal ATTACHMENTS Hip Bone- Femur -.
7. posterior view of right hipischiofemoral ligamentHip LigamentsResists adduction and internal rotation.Note: none of these ligaments restrict flexion.
8. ILIOFEMORAL LIGAMENTLigament of Bigelowstrongest Y shapedStemMedial (vertical)Lateralband(oblique)intermediate thin stratum. Anteriorly blends with capsulePrevents hyperextension of hip
9. PUBOFEMORAL LIGAMENTResists abduction and some external rotation.Base –iliopubic eminence,superior pubic ramus,obturator crest.Blends with capsule deep to medial band of iliofemoral.
10. ISCHIOFEMORAL LIGAMENTWeak Supports capsule from behindFrom ischium, fibres spiral behind femoral neck attach to greater trochanter
11.
12. OTHER LIGAMENTS ABA-Round lig/lig.teres femorisB-Acetabular labrum C-transverse acetabular ligamentC
13. STABILITY OF HIP JOINTDepth of articular socketStrong lig.-Muscles-Length ,obliquity of femur neck.
14. BURSAE AROUND HIP JOINTSubgluteal/ischial bursaSubpsoas/iliopsoas
15. ARTERIAL SUPPLYMedial circumflex femoralLateral circumflex femoral Obturator artery Superior Inferior gluteal Nutrient artery
16. NERVE SUPPLY
17. MOVEMENTS AND RANGE
18. FLEXORSEXTENSORS
19. ABDUCTORSADDUCTORS
20. LATERAL ROTATORSMEDIAL ROTATORS
21. APPLIED ASPECTSDislocation(congenital,acquired)Perthes disease(pseudocoxalgia)Coxa vera and coxa valgaOsteoarthritisFracture neck femur
22. CONGENITAL DISLOCATIONLoose joint capsule Hypoplastic head Externally rotated short limb Inability to abduct Assymmetry of skin folds of thigh
23. AQUIRED DISLOCATIONPosterior(most common)Joint flexed, adducted, medially rotated –Traumatic- Car driver, dashboard strike-Femur head forced out of acetabulum ,capsule tear is posterioinferiorly.
24. PERTHES DISEASEDestruction,flattening of head of femurIncreased joint space
25. COXA VARAIn case of Fracture femur neckPerthes disease
26. COXA VALGASeen in congenital dislocation of hip,rickets- softening neck of femur
27. OSTEOARTHRITISOld ageOsteophytes grow on articular ends- painful, limiting movement .
28. FRACTURE NECK OF FEMURIntracapsular-Subcapital(avascular necrosis most common)CervicalBasal/intertrochantric Extracapsular-old age
29. SHENTON’S LINEIn case of dislocation and in fracture neck femur.DISRUPTED CURVE
30. TRENDELENBURG SIGN
31. SHOEMAKER’S LINEStraight line from tip of greater trochanter to ASIS upto umblicus.If G.T. elevated in fracture neckLine passes below umblicus.
32. MCQ’S
33. Iliofemoral ligament takes origin fromA. Iliopubic ramiB. Posterior inferior iliac spineC. Anterior superior iliac spineD. Anterior inferior iliac spine
34. Lurching gait is seen and trendelenburg sign is positive in paralysis of all EXCEPTA. Gluteus maximus B. Gluteus minimusC. Gluteus mediusD. Tensor fasciae latae
35. Amongst the following muscles which muscle is a medial rotator of thighA. Quardratus femorisB. PiriformisC. Gluteus mediusD. Obturator internus
36. The hip joint most commonly dislocates in the following directionA. anteriorB. posteriorC. superior D. inferior
37. Hyperextension at hip joint is prevented byA. Iliofemoral ligamentB. Ischiofemoral ligamentC. Pubofemoral ligamentD. Capsular ligament