
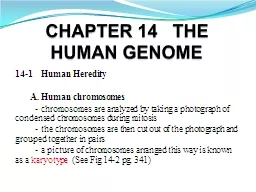
41 Learning ObjectivesLevel I At the end of this unit of study the student should be able to Define chromosome and mitosis List the basic steps of cytogenetic analysis and select the most appropriate type of specimen for analysis of suspected constitutional and neoplastic acquire ID: 919359
Download Presentation The PPT/PDF document "Chromosome Analysis of Hematopoietic and..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
Chromosome Analysis of Hematopoietic and Lymphoid Disorders
41
Slide2Learning Objectives—Level IAt the end of this unit of study, the student should be able to:Define chromosome and mitosis.List the basic steps of cytogenetic analysis, and select the most appropriate type of specimen for analysis of suspected constitutional and neoplastic (acquired) disorders.
continued on next slide
Slide3Learning Objectives—Level IAt the end of this unit of study, the student should be able to:Identify two major types of chromosome abnormalities, describe how they occur, and use the appropriate terminology to describe them.List the practical uses of cytogenetics in the diagnosis and prognosis of hematolymphoid disorders.
Slide4Learning Objectives—Level IIAt the end of this unit of study, the student should be able to:Describe chromosome morphology and mitosis.Determine which specimen type is most appropriate for various clinical indicationsDescribe each step of the cytogenetic harvest procedure.Define and compare aneuploidy, nondisjunction, and anaphase lag.
continued on next slide
Slide5Learning Objectives—Level IIAt the end of this unit of study, the student should be able to:Define and compare translocation, deletion, inversion, and isochromosome.Identify the general categories of hematopoietic disorders for which cytogenetic analysis is useful for patient care.
continued on next slide
Slide6Learning Objectives—Level IIAt the end of this unit of study, the student should be able to:Correlate diagnostic chromosome aberrations with types of hematolymphoid disorders, and assess their prognostic and therapeutic implications.Assess the prognostic impact of cytogenetic results in lymphoblastic leukemia (acute-lymphoblastic leukemia, ALL).
continued on next slide
Slide7Learning Objectives—Level IIAt the end of this unit of study, the student should be able to:Explain the clinical utility of cytogenetics in transplantation.Correlate chromosome abnormalities with specific oncogene activation, and assess the role of the oncogene in the neoplasm.
Slide8CytogeneticsDefinitionStudy of chromosome structure and numberRelated to normal and pathologic statesChromosomal analysisCritical component in patient diagnosis and prognosis for malignant disease
Slide9Chromosome Structure and Morphology
Slide10Chromosome Structure and Morphology Nuclear chromatin of human cells Composed of nucleic acid and protein Organized into 46 chromosomesNucleic acids (DNA and RNA)Composed of polynucleotides
Slide11Chromosome Structure and Morphology Single nucleotide consists of a:PhosphateSugar Deoxyribose for DNA, ribose for RNA
continued on next slide
Slide12Chromosome Structure and Morphology Single nucleotide consists of a:BasePurine—adenine, guaninePyrimidine—cytosine, thymine (DNA)Uracil (RNA)Aligned on the polynucleotide strand in a tripletThree bases code for a single amino acid
continued on next slide
Slide13Chromosome Structure and Morphology Succession of bases in triplet codeDetermines protein productsTranscription of DNATranslation of messenger RNA~ 30,000 genes in human cellsEach located at a specific site in a specific chromosome (gene locus)Alleles—different possible expressions of a gene
Slide14Chromosome Structure and Morphology DNADouble-stranded helix with two polynucleotide strandsHeld together by hydrogen bonds between complementary bases
continued on next slide
Slide15Chromosome Structure and Morphology DNADouble helix initially coils around histone proteins.NucleosomesForm a superhelix—with the six nucleosomes per turn forming a chromatin fiber (solenoid)The fibers are looped back and forth on a protein-RNA scaffold to form an identifiable chromatid.
Slide16Figure 41-1 Chromosome morphology and ultra-structure. (a) Molecular structure of DNA with two polynucleotide chains held together by hydrogen bonding of base pairs (T = thymine, C = cytosine, A = adenine, G = guanine) (b) Double helical structure of DNA. (c) Coiling of double helix strand around histone proteins to produce nucleosome. (d) Superhelix of nucleosome producing chromatin fiber. (e) Coiling of chromatin fiber to produce chromomere. (f) Final structure of chromosome consisting of two identical sister chromatids (condensed chromomere) held together at the centromere.
Slide17Chromosome Structure and Morphology After DNA replicationIdentical sister chromatids are connected at the centromere.Final structure of a mitotic chromosomeCentromereDivides chomosomes into:Short p armsLong q arms
Slide18Chromosome Structure and Morphology Metacentric chromosomep = q1, 3, 16, 19, 20Submetacentric chromosomep < q2, 4, 5, 6–12, 17, 18, X
Slide19Chromosome Structure and Morphology Acrocentric chromosomep is very short, centromere located close to end13–15, 21, 22, and Y
Slide20Figure 41-2 Chromosome structure of a typical submetacentric chromosome and an acrocentric chromosome. The short arm is known as “p” and the long arm as “q”.
Slide21Chromosome Structure and Morphology Satellite DNAArea of chromosome around the centromereContains highly repetitive DNA in long clusters of tandem repeatsPermanently coiled tightly into heterochromatin
Slide22Chromosome Structure and Morphology HeterochromatinStains darkly and is transcriptionally inactiveEuchromatinAreas stain lightly and are transcriptionally active during interphase
Slide23Chromosome Structure and Morphology Normal human cell46 chromosomes—23 pairs1–22 autosomesX and Y sex chromosomesHomologous chromosome pairConsists of two morphologically identical chromosomes that have identical gene loci Can have different alleles
continued on next slide
Slide24Chromosome Structure and Morphology Normal human cellHeterologous pairX and Y chromosome
Slide25MitosisProliferative divisionSeries of stages called the cell cycleG1, S, G2, and mitosisInterphaseCell is not dividing but performing its function.
Slide26MitosisInterphase begins at phase G1.Nuclear chromatin is dispersed.Chromosome morphology is not identifiable.
Slide27MitosisS phaseDNA synthesisDNA replicatedIdentical sister chromatids are attached at the centromere.G2Short resting phaseCell enters mitosis.
Slide28Figure 41-3 Diagram of the cell cycle beginning with G1, the stage in which the cell is performing its designated duties. The DNA is uncoiled and exists as 46 single chromatids. S phase is the time of DNA synthesis after which the DNA is still uncoiled and consists of 46 chromosomes (sister chromatids joined at the centromere). G2 is a resting phase followed by mitosis.
Slide29MitosisProcess of division of somatic cellsEach daughter cell ends with the same genetic composition as the parent cell.
Slide30MitosisProphaseFirst stageDNA begins to coil.Chromosome morphology becomes recognizable.Centrioles, attached to mitototic spindleMigrate to opposite poles of cell
Slide31MitosisMetaphaseDNA is tightly coiled.Chromosomes align in center of cell (equatorial plate).Mitotic spindle apparatus attaches to the kinetochores of the chromosome centromere via microtubules.
Slide32MitosisAnaphaseContraction of spindle fibersPull apart sister chromatidsOne migrates to pole, the other to the other pole.
Slide33MitosisTelophaseDaughter nuclei begin to form at opposite poles.Cytokinesis beginsDivision of the cytoplasm into two daughter cellsCytokinesis completesEach daughter cell re-enters the G1 phase.
Slide34Figure 41-4 Mitosis. (a) Interphase. Chromatin is dispersed. (b) Prophase. Chromosome structure is discernible and centrioles begin to migrate. (c) Metaphase. Chromosomes are lined up in the center, spindle fibers from the centrioles connect to the centromeres, and the nuclear membrane is not visible. (d) Anaphase. Spindle fibers contract and sister chromatids migrate to opposite poles of the cell. (e) Telophase. Chromatid migration is complete and the cytoplasmic membrane forms down the center, completing the cell division.
Slide35MeiosisSpecialized division of diploid primary gametocytesResults in each gamete (oocyte and sperm) having a haploid number of chromosomes
Slide36Cytogenetic Procedures
Slide37Specimen PreparationSpecimensMust have viable cells capable of undergoing mitosisConstitutional cytogenetic aberrationsPresent in every cell in a patient's bodyPeripheral blood most appropriate specimen
continued on next slide
Slide38Specimen PreparationSpecimensAcquired aberrationsHappen after birth in a single cellNeoplastic processesPeripheral blood, BM, tumor biopsies
Slide39Table 41-1 Appropriate Specimens for Cytogenetic Analysis
Slide40Specimen PreparationCytogenetic procedureInduce cells into mitosis."Harvested"Processes cells that are mitotically activeVisualize the chromosomesStepsInduce mitosis.Inhibition of mitotic cells in metaphaseHypotonic incubationFixation
Slide41Harvest Procedure and BandingMitotically active cellsStopped in metaphase Incubate with agents that disrupt spindle apparatusCells incubated with hypotonic solutionHemolyzes RBCs and partially swells nucleated cells
continued on next slide
Slide42Harvest Procedure and BandingMitotically active cellsFixation of cells—Carnoy's fixativeThree to four drops of final cell suspension is placed on slide.
continued on next slide
Slide43Harvest Procedure and BandingMitotically active cellsDried and examined with phase microscopyRemainder of cells prepared, "aged" for banding
Slide44Harvest Procedure and BandingChromosome bandingObtained by various staining proceduresResult in specific pattern of dark-to-light stained bands for each homologous chromosome pair
Slide45Table 41-2 Cytogenetic Banding Techniques and Special Procedures
Slide46Harvest Procedure and BandingFluorescently labeled DNA probes (fluorescence in situ hybridization (FISH)Specific chromosome centromeresWhole armsWhole chromosomesIndividual genes
Slide47Harvest Procedure and BandingFluorescent labeled probesSpecific identification of chromosomes involved in structural or numerical aberrations and analysis of interphase cellsLabeled probe hybridized directly to cells mounted on glass slidesProbe binding visualized by fluorescent microscope
Slide48Chromosome AnalysisPerformed microscopicallyAdequacy of analysis depends on Mitotic rate of the cellsBanded chromosome morphologyOptimal preparationMitotic spreads with moderately long chromosomesFew chromosome overlapsGood quality banding
Slide49Figure 41-5 Metaphase spread of chromosomes belonging to a single cell obtained by direct harvest of a bone marrow aspirate (G-banded, 1000× magnification).
Slide50Chromosome AnalysisKaryotypeRepresentation of the chromosome makeup of a cellConstructed using video-computer-linked analysis system
continued on next slide
Slide51Chromosome AnalysisKaryotypePreparationChromosomes are grouped. Initially by size and centromere positionThen by specific pattern of dark-to-light banding
Slide52Figure 41-6 Karyotype of normal male cell with numbered chromosome pairs, G-banded.
Slide53Chromosomal Abnormalities
Slide54Chromosomal AbnormalitiesAbnormalities—numerical or structuralAutosomes and/or X and Y sex chromosome
Slide55Chromosomal AbnormalitiesConstitutional abnormalitiesPresent at birthPresent in all cells if:Inherited from a parent carrierOccurred during gametogenesisCan also occur shortly after fertilizationMosaic—some cells have aberration and some are normal.
Slide56Chromosomal AbnormalitiesAcquired abnormalitiesOccur sometime after birthUsually seen in a single cellNeoplastic clone
Slide57Numerical AberrationsDiploidNormal human cell—46 chromosomesHaploid (n)Half the number of chromosomes—232n (2 × 23) has 46 chromosomes. (diploid)AneuploidChromosome count other than 46 that is not a multiple of n.
Slide58Numerical AberrationsHyperdipolid > 46 chromosomesHypodiploid < 46 chromosomes
Slide59Numerical AberrationsNondisjunctionMost numerical aberrationsOccurs during meiotic or mitotic cell divisionSpindle fiber from the centromere does not connect to the chromosome centromere.Spindle fiber connects but does not contract.
continued on next slide
Slide60Numerical AberrationsNondisjunctionOne daughter cell with an extra chromosome—trisomyOne daughter cell with a chromosome loss—monosomy
Slide61Figure 41-7 Nondisjunction. During anaphase, the sister chromatids of a chromosome do not disjoin, resulting in one daughter cell with an extra chromosome (trisomy) and the other with a chromosome loss (monosomy).
Slide62Numerical AberrationsAnaphase lagOne chromatid does not completely migrate to the opposite pole.Lags behind—gets caught outside the nuclear membraneOne daughter cell with a chromosome lossOne normal daughter cell
Slide63Figure 41-8 Anaphase lag. Chromatid does not complete migration, resulting in one daughter cell with a normal chromosome count and the other with a chromosome loss.
Slide64Numerical AberrationsEndomitosisPolyploid cells Multiple rounds of S phase without karyokinesis or cytokinesisMegakaryocytes
Slide65Numerical AberrationsPseudodiploid 46 chromosomesNot normal due to numerical/structural abnormalitiesExample: 46, XX, +8, −21
Slide66Structural AberrationsChromosome breakage occursRepair process results in structural loss or abnormal recombinationsConstitutional or acquired
Slide67Table 41-3 Examples of Structural Chromosome Aberration Nomenclature with Explanations
Slide68Polymorphic VariationMorphologic variationsOccur in certain chromosomesNo clinical significanceIf present, is inherited consistently through each generationEasily demonstrated with various banding techniquesUsed to ID maternal vs. paternal origin
Slide69Cytogenetic Nomenclature
Slide70Cytogenetic NomenclatureStandard nomenclature system Chromosome number, region, band, and karyotypeShort and long arms of each chromosome divided into regions by landmark bands
continued on next slide
Slide71Cytogenetic NomenclatureStandard nomenclature system Further region divided into distinct light-, intermediate-, and dark-staining bandsNumbering of regions and bands begin at the centromere
continued on next slide
Slide72Cytogenetic NomenclatureStandard nomenclature systemProceeds distally to the terminal portions, pter, and qterIn each region, numbering of bands begins with one.Specific band of chromosome Chromosome #, arm, region, band
Slide73Figure 41-9 Diagram of bands on chromosome 7 with arm, region, and band designations. The band located at the arrow is designated 7q32.Short arm = p; long arm = q
Slide74Cytogenetic NomenclatureStandard nomenclature for gene namesKaryotype of cellTotal # of chromosomesSex chromosome, XX, XY
Slide75Cytogenetic NomenclatureKaryotype of cellIf aberrations are present:Sex chromosomes aberrations firstAutosome aberrations—in numerical orderNumerical + or - before chromosome numberStructural—appropriate abbreviation, chromosome involved in parenthesis, break point designation in parentheses
Slide76Cytogenetic NomenclatureExamplesNormal male 46, XYNormal female 46, XXMale cell with trisomy chromosomes 8 and 21 48,XY,+8,+21
continued on next slide
Slide77Cytogenetic NomenclatureExamplesFemale cell with trisomy for chromosomes 3, 8, 15 and a translocation involving chromosome 9 and 2249,XX,+3,+8,t(9;22)(q34;q11.2),+15
Slide78Cytogenetic Analysis of Hematopoietic and Lymphoid Disorders
Slide79Cytogenetic AnalysisEssential For diagnosis and prognosis of hematolymphoid malignancies and solid tumorsChromosomal aberration in neoplastic cellsAcquired, clonal aberrationOccurs sometime after birthPresent only in neoplastic cells
Slide80Cytogenetic AnalysisChromosomal aberration in neoplastic cellsClone existsNumerical and/or structural aberrations are identical in at least two cellsMonosomy—three cells must have identical aberration
Slide81Table 41-4 Present Applications of Conventional Cytogenetics and Molecular Cytogenetics (FISH) in Hematolymphoid Disorders
Slide82Processing of SpecimensBone marrow aspirateBest sample for cytogenetic analysis of hematolymphoid disorders, excluding lymphomasCells processed by Direct harvest and/or unstimulated culturesOptimal cultures obtained by inoculating one million cells per milliliter of media
Slide83Processing of SpecimensLymph nodeBest sample for lymphoma
Slide84Table 41-5 Appropriate Specimens and Type of Processing for Cytogenetic Analysis of Neoplastic Cells
Slide85CML90–95% of patients with CMLChromosomal abnormality of a balanced translocationChromosomes 9 and 22t(9;22)(q34;q11.2)
Slide86CMLChromosomal abnormality Proto-oncogene ABL1—normally located at 9q34Translocated and juxtaposed next to the BCR gene at 22q11.2 in the Philadelphia translocation
Slide87CMLPh chromosomeResults in a new chimeric gene consisting of:Portion of ABL1 from chromosome 9Portion of BCR from chromosome 22ABL1 is activated to a functioning oncogene.210 kD polypeptide product BCR/ABL1 is present in leukemic cells.
Slide88CML5—10% patients lack Ph t(9;22)Variant translocationCryptic translocationNeed molecular technique such as FISH for BCR/ABL1
Slide89CMLTreatmentDeveloped agent targeted specifically at the protein product of the ABL1 geneTyrosine kinase inhibitors (TKIs)Patients enter accelerated phase or blast crisisChange in karyotypeChromosome aberrations in addition to t(9;22)
Slide90Figure 41-10 Identification of the BCR/ABL1 gene rearrangement with a dual color, dual fusion probe set. The ABL1 probe is labeled in red and the BCR probe in green. One normal ABL1 gene and one normal BCR gene are located on separate chromosomes. The BCR and ABL1 genes are juxtaposed on the two chromosomes involved in the translocation, resulting in two yellow fusion signals.
Slide91t(9;22)15% of ALLMore common in adultsDifference in site of breakage of the BCR locus190 kD proteinPh+ ALL must be differentiated from lymphoid blast crisis of CML
Slide92Myeloproliferative Disorders Other Than CMLClonal chromosome aberrations50–60% of casesMyeloproliferative disorders Polycythemia vera (PV)Chronic idiopathic myelofibrosis Essential thrombocythemia (ET)Diagnosis of these disordersDocumented absence of BCR/ABL1 gene arrangement
continued on next slide
Slide93Myeloproliferative Disorders Other Than CMLClonal chromosome aberrationsRecurrent aberrationsAbnormalities of 1q, +8, +9, del(13q), and del(20q)Molecular genetic evaluation for JAK2 gene (V617F mutation)High response rate to hydroxyureaShorter overall survival
Slide94Acute Myeloid Leukemia De novo AMLAcquired clonal chromosome aberrations in the leukemic cells in 70% of cases Aberation present only in leukemic cellsChromosome abnormalities can be Single, numerical, structural, complex
Slide95Acute Myeloid Leukemia WHOClassification system for AML according to presence or absence of recurrent cytogenetic abnormalitiesSpecific aberrations define AML subtypes
Slide96Acute Myeloid Leukemia t(8,21) and inv(16)/t(16;16)Disrupt transcription factor—core binding factor (CBF)Favorable prognosest(15,17)Fusion of RARA gene at 17q21.1 with PML gene at 15q24.1Respond to treatment with ATRAInduces differentiation of promyelocytes
Slide97Acute Myeloid Leukemia t(8;21), inv(16), and t(15;17)Considered acute leukemias regardless of blast count
Slide98Acute Myeloid Leukemia AML with myelodysplasia-related changesBlast count > 20%Morphologic features or history of MDS, MDS-related cytogenetic abnormalities and absence of aberrations seen in AML with recurrent genetic abnormalitiesOften include aberration in five and sevenPoor prognosis
Slide99Acute Myeloid Leukemia Secondary or therapy-related AMLAlkalating agents—aberrations of five and sevenTopoisomerase II inhibitors—break points at band 11q23 and concurrent MLL gene rearrangement
Slide100Myelodysplastic Syndromes (MDS)International Prognostic Scoring System (IPSS)Predicts survival of MDS patients and transformation to AMLVariablesType of cytogenetic abnormality% blastsDegree and number of cytopenias
continued on next slide
Slide101Myelodysplastic Syndromes (MDS)IPSSGood risk cytogeneticsNormal karyotype, del(5q) as sole abnormality, del(20q) as sole abnormality, and –YPoor risk cytogenetics:≥ three chromosome aberrations and chromosome 7 abnormalities Intermediate risk refers to all other abnormalities.
Slide102Acute Lymphoblastic Leukemia (ALL)Clonal acquired aberrations60–75% of patients
Slide103Acute Lymphoblastic Leukemia (ALL)Cytogenetic findings important in pediatrics Favorable prognosisHyperdiploid karyotypes (54–65 chromosomes)Trisomies of 4, 10, 17t(12;21)(p13;q22.3)
continued on next slide
Slide104Acute Lymphoblastic Leukemia (ALL)Cytogenetic findings important in pediatrics Poor prognosisHypodiploidy, t(4;11)(q21;q23), t(9;22) (q34.1;q11.2)
Slide105Lymphoma and Lymphoproliferative DisordersCytogenetic aberrations Associated with specific types of lymphomaMajor diagnostic and prognostic significance
continued on next slide
Slide106Lymphoma and Lymphoproliferative DisordersCytogenetic aberrations Most translocations Known to involve genes that are critical for:Proliferation of the neoplastic cellsInvolved in programmed cell death, apoptosis
Slide107Bone Marrow TransplantationCytogenetics, particularly FISH analysisValuable tool in evaluating rate of engraftment of donor cells in opposite sex transplants Monitoring for minimal residual disease
Slide108Bone Marrow TransplantationAfter donor transplantationOnly donor cells should be present.If recipient cells recur with a normal karyotypeIndicates the development of a chimerismPresence of cells of two different genetic origins in an individual
Slide109Molecular CytogeneticsFISH and cytogenomic microarray analysis (CMA)Evaluate individual gene compositionAdvantageDoes not require viable cells capable of mitotic activity
continued on next slide
Slide110Molecular CytogeneticsFISH and cytogenomic microarray analysis (CMA)DisadvantageGive info about a single molecular genetic aberration based on specific probe usedMay miss other aberrations.
Slide111Molecular CytogeneticsCytogenomic microarray analysis (CMA)Used to analyze changes in chromosome copy numberUse single nucleotide polymorphisms (SNPs)Allow absence of heterozygosity (AOH) to be detectedFrequent finding in cancer specimensFuture diagnostic utility
Slide112Chapter 41—Case Study25-year-old man, GregoryRoutine physical exam and lab studies for new employmentWBC 30,000 × 109/LConsider what conditions may result in this clinical picture and the follow-up studies that should be done.
continued on next slide
Slide113Chapter 41—Case StudyDifferential7% blasts 3% promyelocytes 25% myelocytes 10% metamyelocytes 5% bands25% segs10% basophils
continued on next slide
Slide114Chapter 41—Case StudyDifferential5% eosinophils10% lymphocytesDifferential diagnosis includes leukemoid reaction, CML, MPDs other than CML. BM aspirate is performed.
continued on next slide
Slide115Chapter 41—Case StudyQuestion 1:What is the most appropriate specimen to submit for cytogenetics, and how should it be processed?Cytogenetic analysis of BM shows all of the cells to have this karyotype:46,XY,t(9;22)(q34;q11.2)
continued on next slide
Slide116Chapter 41—Case StudyQuestion 2:Is this a constitutional or acquired aberration?Question 3:Is it a clonal aberration?Question 4:What is the significance of this finding for the diagnosis?
continued on next slide
Slide117Chapter 41—Case StudyAn allogeneic BM transplant is performed with Greg's sister as the donor.Three months after transplantKaryotype 46,XXQuestion 5:What is the significance of this finding?
continued on next slide
Slide118Chapter 41—Case StudySix months after transplantBM was performed.Mitotic yield of the specimen was not sufficient for routine cytogenetic analysis.Question 6:What other studies that would be informative as to the status of the donor and recipient cells could be performed?
continued on next slide
Slide119Chapter 41—Case StudyQuestion 7:Five years after the transplant, cytogenetic analysis shows the following:5 cells—46,XX15 cells—47,XY,+8,t(9; 22)(q34; q11.2), i(17)(q10)What is the significance of these findings?