
Increase frequency of urine gt1500mlday Causes Diabetes mellitus Acrete Nephritis Nephrotic syndrome Post Pitutary tumour 2 Oliguria Decrease frequency of urine lt 500 mlday ID: 913325
Download Presentation The PPT/PDF document "Renal System 1. Polyurea" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
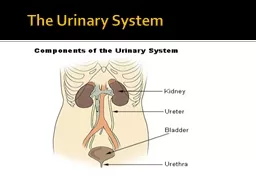
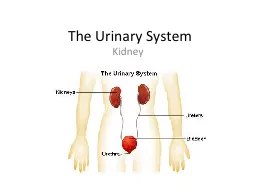
Renal System
1.
Polyurea
(Increase frequency of urine) >1500ml/day
Causes . Diabetes mellitus
.
Acrete
Nephritis / Nephrotic syndrome
. Post
Pitutary
tumour
2. Oliguria (Decrease frequency of urine) < 500 ml/day
3. Anuria (Absence of formation of urine)
Causes of oliguria & Anuria
. Pyrexia & Excessive sweating
. Vomiting, Loose motion, Dehydration
. Hypovolaemia
. Prostatic hypertrophy
.
Chronic Renal failure
.
CHF
.
Stricture in urinary bladder (Stone etc.)
Slide24. Nocturia (Increase frequency of urine at Night)
. Diabetes Mellitus
. HTI
5. Haematuria:
True
Haematurea
False
Haematurea
Macroscopic
Haematures
Microscopic
Haematures
.
True
Haematurea
– Colour of urine is red and RBCs are present in urine (200 > 2RBC)
False
Haematurea
– Colour of
urine is red
but RBC are not present in urine.
Cause
– By eating Beat root
– Rifampicin
–
Pyridium
Slide3True Haematurea
Painful
Haematurea
Painless
Pre
Micturation
Haematurea
With
Micturation
Haematurea
(Mixed)
Post
Micturation
Causes –
Pre
Micturation
Haematurea
.
Urethal
Causes (Injury)
. BPH
–
With
Micturation
Haematurea
(Mixed)
.
Ureteric Causes (Stone)
Slide4. Renal Causes
. Stone
.
Polycustic
Kidney
. Glomerulonephritis
.
Malignaut
tumour in Kidney
. T.B. of Kidney
Post
Micturation
Haematurea
. Any cause in urinary bladder
. Cystitis
. Vesical Calculus
. CA of Urinary Bladder
Extra Renal Causes
. SABE
. Appendicitis
.
Salfringitis
. Diverticulitis
Slide56. Retention of Urine: It should be differentiated from
Anurea
/ oliguria. In retention of urine kidney function is normal while oliguria & Anuria indicate towards disturbed function of the kidney.
Causes :
. Urethral obstruction
. Urethral Stricture
. Pin hole meatus (Esp. in children)
.
Phymosis
. Prostatic hypertrophy
. Spinal causes.
Slide67. Incontinence of urine: Improper involuntary passage of urine resulting is wetting.
Causes:
. Common in old age (due to damage of brash cells)
. Common in
Multipase
(due to weakening of muscles)
. In
paraplagis
(lower body paralysis)
. Pressure on bladder
8. Pain in Renal angle or
lein
:
(Angle between 12
th
rib & Erector
spinaemus
).
Causes
. Inflammatory condition in Kidney (i.e., stone)
. It is colicky in nature
. It is in agony and in restless condition pain goes from loin to groin, scrotum, glans,
labias
.
Slide7Signs1. Oedems
:
.
Oedems
of Renal origin starts from face. (
Peri
or
bitaol
oedems
)
.
Oedems
of Cardiac origin starts from legs.
.
Oedems
of
Heptic
origin starts from abdomen.
2. Rashes on skin : seen in Uraemia
Breath smell : seen in Uraemia / Renal failure
3. Nails : Half
Half
nails seen in Renal failure.
Ben’s line (
Transverseriolgeson
nail – chronicity of dis.)
4. Ascites.
5. Signs of Hypertension (if Renal cause)
Slide8Inspection1. Oedems
/ Generalised
anasarce
in Acute Renal failure.
2. Skin: Rough, Dry, Dark brown with scratches & wrinkles in chronic
Renal failure.
3. Nails: White & Opaque nails in chronic Renal failure.
Palpation
Palpation of kidney by
Bimannual
method. Generally Kidney are not palpable.
palpable kidney indicates:
.
Hydronephrosis
(May be unilateral)
. Polycystic Kidney (Always Bilateral)
Slide9Persussion
. Fluid thrill
. Shifting dullness
. Pleural effusion may be in Nephrotic syndrome.
Anscultration
. Bruit (on
Renala
)
Indicates stenosis of
Renala
.
(If this sound is heard over the heart, it is called murmur.)
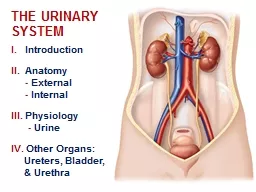
Slide10Investigation of Renal system1. Urine test
Physical examination
. Normal amount (It may vary from 700-2500ml)
. Specific gravity (1.003-1.030)
. Odour
Chemical Examination
. Protein
. Ketone bodies
. Bile salts
. Bile pigments.
Microscopic Examination
. RBS
. Pus Cells
. Cast (
Hyalina
Cast indicates
Glomerulonephrites
)
. Crystals
Urine Culture &
Sensitivity
2. R&T (Renal function test)
. Blood urea (Normal 20-40 mg / 100ml)
. Serum Creatinine (0.5 mg – 1.2 mg)
Slide11Radiological Investigation1. Plane X-ray abdomen for KUB (Kidney, Ureter, Bladder)
2. IVU (Intravenous Urography)
3. IVP Intravenous Pyelography)
for kidney function.
4. USG (Ultra Sonography)
5. C.T. Scan
6. Cystography
7.
Urethrography
8. MRI (
Magnatic
Resonant Imaging
)