
in Patients with Endstage Renal Disease on Hemodialysis Sarah Nisivaco 1 Brooke Patel 1 Kaitlin Grady 1 Husam H Balkhy 1 1 Department of Surgery University of Chicago Medicine Chicago IL USA ID: 915728
Download Presentation The PPT/PDF document "BACKGROUND Outcomes of Robotic Totally E..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
BACKGROUND
Outcomes of Robotic Totally Endoscopic Coronary Artery Bypass
in Patients with End-stage Renal Disease on Hemodialysis
Sarah Nisivaco1, Brooke Patel1, Kaitlin Grady1, Husam H Balkhy11Department of Surgery, University of Chicago Medicine, Chicago, IL, USA
Husam H Balkhy is a proctor for Intuitive Surgical.
The presence of end stage renal disease (ESRD) is known to confer a negative impact on outcomes of patients undergoing coronary bypass surgery. Notably, a higher short-term mortality has been consistently demonstrated. [1,2] We hypothesized that robotic-assisted totally endoscopic beating-heart coronary bypass (TECAB), which is the least invasive form of surgical coronary revascularization, may have a positive impact on these outcomes. The objective of this study was to evaluate the short and mid-term outcomes in patients with ESRD on hemodialysis (HD) who underwent this procedure at our institution.
The benefits of coronary artery bypass (CABG) over percutaneous coronary intervention in ESRD patients on HD including lower mortality, have been demonstrated. [1,2] However, ESRD historically confers a higher risk in patients undergoing conventional coronary bypass grafting. [3] In addition, these patients demonstrate worse long-term outcomes, even with coronary revascularization, due to their underlying comorbidity. [4,5] Our study demonstrates that beating-heart robotic TECAB is feasible and safe for patients on HD with coronary artery disease. The early outcomes were comparable to patients with normal renal function and are superior to outcomes of traditional CABG in this challenging group of patients. [3] Further long-term studies are warranted.
PATIENTS AND METHODS
RESULTS
RESULTS
DISCLOSURES
Study Design
Retrospective cohort study of 486 beating heart TECAB patients, July 2013 – December 2019
Cohorts: ESRD on HD (N = 22) and Non-HD (N = 464)Exclusion criteria for beating-heart TECAB include emergency surgery, cardiogenic shock, and fused left pleural space.
REFERENCES
1. Ix JH, Mercado N, Shlipak MG, et al. Association of chronic kidney disease with clinical outcomes after coronary revascularization: the Arterial Revascularization Therapies Study (ARTS). Am Heart J 2005;149: 512-9.2. Charytan DM, Yang SS, McGurk S, et al. Long and shortterm outcomes following coronary artery bypass grafting in patients with and without chronic kidney disease. Nephrol Dial Transplant 2010;25: 3654-63. 3. Mourad F, Cleve N, Nowak J, et al. Long-Term Single Centre Outcomes of Patients with Chronic Renal Dialysis Undergoing Cardiac Surgery. Ann Thorac Surg. 2019 Sep pii: S0003-4975(19)31432-8. doi: 10.1016/j.athoracsur.2019.08.042. [Epub ahead of print]4. Chang TI, Shilane D, Kazi DS, Montez-Rath ME, Hlatky MA, Winkelmayer WC. Multivessel coronary artery bypass grafting versus percutaneous coronary intervention in ESRD. J Am Soc Nephrol. 2012;23(12):2042‐2049. doi:10.1681/ASN.2012060554 5. Zheng H, Xue S, Lian F, Huang RT, Hu ZL, Wang YY. Meta-analysis of clinical studies comparing coronary artery bypass grafting with percutaneous coronary intervention in patients with end-stage renal disease. Eur J Cardiothorac Surg. 2013;43(3):459‐467. doi:10.1093/ejcts/ezs360
CONCLUSIONS
Group CharacteristicsHD Group (N=22)Non-HD Group (N=464)p valueAge (years), mean ± SD60.2 ± 8.266.1 ± 10.30.007Female Gender, n (%)9 (41)114 (25)0.085STS Predicted Mortality, mean ± SD6.16 ± 6.51.47 ± 2.1<0.001Diabetes Mellitus, n (%)18 (82)182 (39)<0.001Hypertension, n (%)22 (100)378 (81)0.026Peripheral Vascular Disease, n (%)10 (45)50 (11)<0.001Congestive Heart Failure, n (%)10 (45)78 (17)<0.001Listed for Organ Transplant, n (%) 4 (18) 7 (1.5)<0.001
Intraoperative Characteristics HD Group (N=22)Non-HD Group (N=464)p valueRobotic Operative Time (min), mean ± SD240 ± 106248 ± 830.717Number of Grafts, mean ± SD1.41 ± 0.591.66 ± 0.620.070Bilateral IMA Use, n (%)6 (27)230 (50)0.041Hybrid Procedure, n (%)14 (64)191 (41)0.049Cardiopulmonary Bypass, n (%)0 (0) 5 (0.7)0.025Conversion to Sternotomy, n (%)1 (4.5)0 (0)0.329Intraoperative Blood Transfusion, n (%)8 (36)28 (6.0)<0.001
Postoperative OutcomesHD Group (N=22)Non-HD Group (N=464)p valueExtubation, n (%) In OR <24 hours >24 hours1 (4.5)20 (91)1 (4.5)234 (50.5)223 (48)7 (1.5)<0.0010.4950.514Hospital LOS (days), mean ± SD3.31 ± 1.42.78 ± 1.30.078ICU LOS (days), mean ± SD1.58 ± 0.81.30 ± 0.690.088Chest Tube Output (mL), mean ± SD631 ± 400616 ± 357 0.852Postoperative Blood Transfusion, n (%)6 (2.7)49 (10.6)0.016Atrial Fibrillation, n (%)3 (14)63 (14)0.994Wound Infection, n (%)0 (0)0 (0)n/aReturn to OR for Bleeding, n (%)0 (0)6 (1.3)0.014Readmission, n (%)3 (14)28 (6)0.161Mortality, n (%)0 (0)5 (1.1)0.025
SURGICAL TECHNIQUE
Table 1. Baseline Characteristics (SD: standard deviation; STS: society of thoracic surgeons)
Table 2: Intraoperative Characteristics (SD: standard deviation; IMA: internal mammary artery)
Table 3. Postoperative Outcomes (OR: operating room; LOS: length of stay; ICU: intensive care unit)
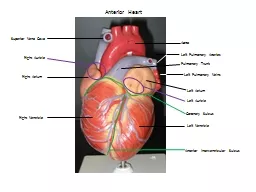
All operations were performed totally endoscopically on the beating heart (without cardiopulmonary bypass) using the da Vinci Si surgical system by the same experienced robotic surgeon and team. Ports were placed in the second, fourth, and sixth interspaces in the anterior axillary line and a 4
th
subcostal port was used for the Endowrist stabilizer. Patients underwent either single or multivessel all arterial bypass grafting with the aid of the Flex-A distal anastomotic device or with a hand-sewn sutured technique.
Mid-Term Outcomes
HD Group (N=22)Non-HD Group (N=458)p valueAverage Time to Follow-Up (months), mean ± SD25.1 ± 18.731.9 ± 21.50.112All Cause Mortality, n (%)9 (41)54 (12)0.013Cardiac-related Mortality, n (%)1 (4.5)11 (2.4)0.450Repeat Cardiac Surgery, n (%)0 (0)7 (1.5)0.008Myocardial Infarction, n (%)2 (9.1)9 (2.0)0.032Freedom from Angina, n (%)22 (100)448 (98)0.585Freedom from MACE, n (%)19 (86)424 (93)0.266Graft Patency during Hybrid Angiogram, n/total grafts evaluated (%)14/15 (93)206/213 (97)0.492
Table 4. Mid-Term Outcomes (PCI: percutaneous coronary intervention; MACE: major adverse cardiac events)