
Pediatric Continuity Clinic Curriculum Created by Matthew Pertzborn PGL2 Objectives Describe the common clinical presentation and diagnosis of atopic dermatitis Understand the management of atopic dermatitis ID: 684724
Download Presentation The PPT/PDF document "Atopic Dermatitis April 2015" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
Atopic DermatitisApril 2015
Pediatric Continuity Clinic Curriculum
Created by: Matthew Pertzborn, PGL-2Slide2
Objectives
Describe the common clinical presentation and diagnosis of atopic dermatitis
Understand the management of atopic dermatitis
Discuss common co-morbidities and complications of atopic dermatitisSlide3
Case #1
A 12 month old female presents with a 6 month history of intermittent
erythema
, dryness, and cracking of the skin on the face and on the extensor surfaces of the arms. She has been scratching at the affected areas.
Question 1-1: What is the differential diagnosis of these symptoms?
Question 1-2: What is the typical distribution of atopic dermatitis?
Question 1-3: What are common triggers of atopic dermatitis?Slide4
Discussion question 1-1?
Differential includes:
Contact dermatitis
Psoriasis
Impetigo
Histiocytosis
X (particularly if the distribution involves the diaper area in children wearing diapers)
Wiskott
-Aldrich syndrome
Scabies
Seborrheic
dermatitis
Drug reaction
Lymphoma with
cutaneous
involvement
Immune system disorder (e.g. hyper-
IgE
syndrome)
Zinc deficiencySlide5
Discussion question 1-2?
It is important to be aware of the typical distribution:
Infants (most common onset is between 3 and 6 months of age)
Face
Extensor
sites
Trunk
Older Children
Flexor sites
Antecubital
fossa
Popliteal
fossa
Neck
Trunk
Typically
spares the groin and
axillary
areas
Stuffy-sounding nose is a common observationSlide6
Discussion question 1-3?
Common triggers/exacerbating factors in atopic dermatitis:
Food/formula
Mechanical
Soaps
Detergents
Wool
Weather (e.g. low levels of humidity)
Diaphoresis
Dust mites (
Dermatophagoides
pteronyssinus
)
Mold
Pollen
Pets
Bacteria
StressSlide7
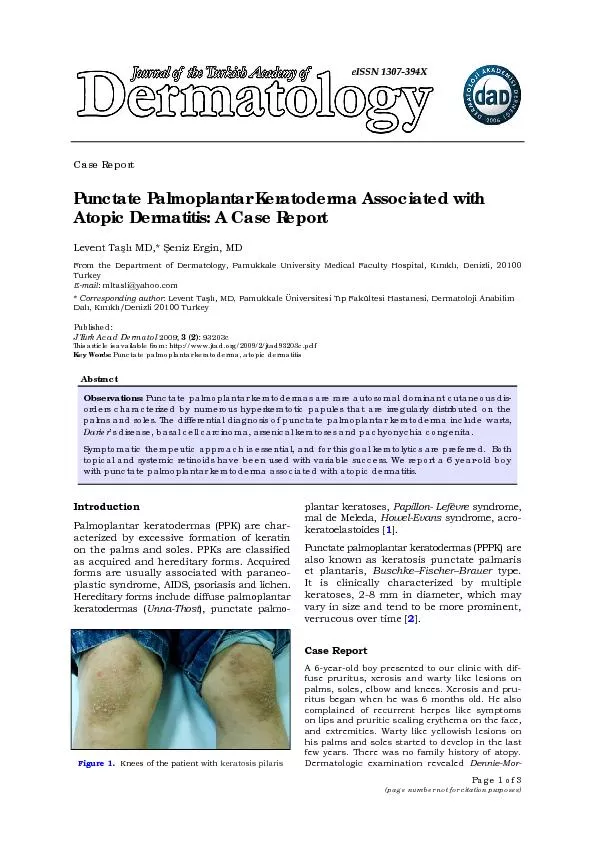
Additional Information
Image From: Pediatrics In Review (Reference #1)Slide8
Additional InformationOften follows a relapsing course
The term “atopic dermatitis” and “atopic eczema” (often simply called “eczema”) are the same
Itching is very characteristic
IgE
often elevatedSlide9
Case #2
A 3 year old male presents with a 2 year history of intermittent
erythema
, dryness, and cracking of the skin on the face and on the extensor surfaces of the arms. The symptoms were previously controlled adequately with application of Vaseline after baths. He has been having multiple flares of these symptoms despite the Vaseline management and the mother is wondering what else can be done.
Question 2-1: What is the first-line management for eczema in general?
2-2: What is the best next treatment choice for the patient above?
2-3: Is there a non-corticosteroid alternative for severe disease?Slide10
Discussion question 2-1?
Initial Management of Eczema:
Removal of potential triggers if possible
Use mild, non-scented soap (e.g. Dove soap) only
Minimize non-soap cleaners
Should be neutral to low pH, fragrance-free, hypoallergenic if used
Removal of certain detergents for washing clothes. Avoid dryer sheets (e.g. Bounce) and detergents with fragrances.
Topical
moisturizers/emollients (e.g. petrolatum jelly,
Aquaphor
ointment)
Ointments more effective than creams
Lotions should be avoided
Application after bath (immediately after drying)
Application throughout the day
Exact frequency and amount not well delineated in the literatureSlide11
Discussion question 2-2?
Management of acute flares if the initial management is not adequate:
Some advocate burst of high-dose corticosteroids with tapering in potency once controlled, others advocate starting with lowest-potency corticosteroids and then titrating upward
Potency ranges from lowest-potency (class VII (e.g. hydrocortisone 0.25-1%)) to high-potency corticosteroids (class I (e.g.
diflorasone
))
Caution should be used when applying higher-potency corticosteroids to the face, neck, or skin-folds as risk of significant systemic absorption is higher in these
areas
Avoid using higher-potency corticosteroids for more than 2 weeks at a time
Typically dosed 2x per daySlide12
Discussion question 2-2?
Management of acute flares if the initial managements are not adequate:
Wet-wrap therapy can be useful as adjunct
Involves covering the area on which the topical moisturizer or topical corticosteroid is applied with a wet bandage and then placing a dry bandage on top of the wet bandage
Wrap may be kept on for up to 24 hours at a time and this adjunct has been used for as much as 2 weeks in the literature
Use of this adjunct with mid- to high-potency corticosteroids is controversialSlide13
Discussion question 2-3?
Topical
calcineurin
inhibitors
May be used to avoid side/adverse effects of corticosteroids, particularly if high-potency corticosteroids are required, skin atrophy secondary to corticosteroid use occurs, or topical corticosteroids are required long-term
Topical
tacrolimus
ointment (0.03-0.1%) or
pimecrolimus
cream (1%)
Typically dosed 2x per daySlide14
Additional InformationClinical pearl:
Important to apply emollient/ointment after every bath (pad down with towel, don’t wipe after the bath prior to application)Slide15
Case #3
A 3 year old male presents with a 2 year history of intermittent
erythema
, dryness, and cracking of the skin on the face and on the extensor surfaces of the arms. Starting 5 days ago, there has been some crusting on the face with a small amount of yellow oozing
What other medical conditions (non-infectious) are associated with eczema?
Are there increased risk of infectious co-morbidities in eczema?
Is there anything that can be done to prevent secondary infection?Slide16
Discussion question 3-1?
Allergic rhinitis, asthma, and food allergies are associated with eczema.
Extra careful screening for the above conditions should occurSlide17
Discussion question 3-2?
Secondary skin infections possible:
Staphylococcus
aureus
most common
Appropriate systemic antibiotic therapy if secondary infection occurs (depends on local resistance profiles)
Clindamycin
Bactrim
If secondary infections frequent:
Mupirocin
to the
nares
if Staphylococcus
aureus
colonization suspected (BID x10 days)
Bleach baths if signs of secondary infection
present (may also do this
prophylactically
if eczema is extensive)
Can reduce colonization
dramatically
1/4-1/2 cup household bleach (6% sodium hypochlorite) in half-filled bath
Stay in bath 20 minutes then rinse with fresh water after
Typically weekly
Lukewarm temperatureSlide18
Additional InformationClinical pearl: Remember to ask about family history of allergic rhinitis (seasonal allergies),
hay fever, asthma
,
and
eczema.
70% of patients with eczema have atopic disease in other members of the familySlide19
PREP Question
PREP 2014 Item 141:
The mother of a 7-month-old infant is frustrated that the infant’s atopic dermatitis is not getting better. He is awake “all night” scratching and is irritable and fussy. She has been giving him
diphenhydramine
every 8 hours and applying hypoallergenic moisturizer and a topical corticosteroid cream twice a day. The infant was breastfed until 3 months ago and then switched to a cow milk-based formula. On physical examination, you notice that he has dry,
erythematous
papules and patches, with excoriation marks on his face, neck,
antecubital
fossae
,
popliteal
fossae
, and back. He has normal growth parameters.
Of the following, the MOST appropriate next step in this infant’s management is to recommend:
A. discontinuing
diphenhydramine
and switching him to daily
loratadine
B. eliminating cow milk, egg, soy, and wheat from his diet
C. Introducing cow milk on a trial basis to see if the rash worsens
D. switching to hypoallergenic formula and a diet of only rice and chicken
E. testing for pertinent, potential food allergen triggersSlide20
PREP Question
PREP 2014 Item 141:
The mother of a 7-month-old infant is frustrated that the infant’s atopic dermatitis is not getting better. He is awake “all night” scratching and is irritable and fussy. She has been giving him
diphenhydramine
every 8 hours and applying hypoallergenic moisturizer and a topical corticosteroid cream twice a day. The infant was breastfed until 3 months ago and then switched to a cow milk-based formula. On physical examination, you notice that he has dry,
erythematous
papules and patches, with excoriation marks on his face, neck,
antecubital
fossae
,
popliteal
fossae
, and back. He has normal growth parameters.
Of the following, the MOST appropriate next step in this infant’s management is to recommend:
A. discontinuing
diphenhydramine
and switching him to daily
loratadine
B. eliminating cow milk, egg, soy, and wheat from his diet
C. Introducing cow milk on a trial basis to see if the rash worsens
D. switching to hypoallergenic formula and a diet of only rice and chicken
E. testing for pertinent, potential food allergen triggers (see PREP 2014 for explanation)Slide21
PREP Question
PREP 2014 Item 106:
The parents of a 3 year old boy would like him to be tested for allergies. The parents report that the boy has had worsening symptoms of itchy eyes, sneezing fits, and nasal congestion since the family got a new dog 1 year ago. The parents would like the boy tested to determine if they need to give the dog away. They are reluctant to stop the boy’s daily antihistamine and are disappointed to learn that skin testing cannot be performed while taking this medication. You decide to obtain blood-specific
IgE
testing. However, the parents have read on the internet that the “scratch test” is a better test. Of the following, you are MOST likely to advise the parents that in this situation, blood-specific
IgE
testing is:
A. Comparable to skin testing
B. Less expensive and better tolerated by children than skin testing
C. More accurate than skin testing
D. The only testing that can be done because he is too young for skin testing
E. A preliminary test and you will obtain skin testing to confirm the resultsSlide22
PREP Question
PREP 2014 Item 106:
The parents of a 3 year old boy would like him to be tested for allergies. The parents report that the boy has had worsening symptoms of itchy eyes, sneezing fits, and nasal congestion since the family got a new dog 1 year ago. The parents would like the boy tested to determine if they need to give the dog away. They are reluctant to stop the boy’s daily antihistamine and are disappointed to learn that skin testing cannot be performed while taking this medication. You decide to obtain blood-specific
IgE
testing. However, the parents have read on the internet that the “scratch test” is a better test. Of the following, you are MOST likely to advise the parents that in this situation, blood-specific
IgE
testing is:
A. Comparable to skin testing (see PREP 2014 for explanation)
B. Less expensive and better tolerated by children than skin testing
C. More accurate than skin testing
D. The only testing that can be done because he is too young for skin testing
E. A preliminary test and you will obtain skin testing to confirm the resultsSlide23
References and Future Reading
Eichenfield
, Lawrence F.,
Wynnis
L. Tom, Sarah L.
Chamlin
, Steven R. Feldman, Jon M.
Hanifin
, Eric L. Simpson, Timothy G. Berger, James N. Bergman, David E. Cohen, Kevin D. Cooper, Kelly M.
Cordoro
, Dawn M. Davis,
Alfons
Krol
, David J. Margolis, Amy S.
Paller
, Kathryn
Schwarzenberger
, Robert A. Silverman,
Hywel
C. Williams, Craig A.
Elmets
, Julie Block, Christopher G.
Harrod
, Wendy Smith
Begolka
, and Robert
Sidbury
. "Guidelines of Care for the Management Of atopic dermatitis."
Journal of the American Academy of Dermatology
70.2 (2014): 338-51. Web.
Cipriani
, Francesca, Arianna
Dondi
, and
Giampaolo
Ricci. "Recent Advances in Epidemiology and Prevention of Atopic Eczema."
Pediatric Allergy and Immunology.
10 Dec. 2014. Web. 28 Dec. 2014.Slide24
References and Future Reading
Knoell
, K. A., and K. E. Greer. "Atopic Dermatitis."
Pediatrics in Review
20.2 (1999): 46-52. Web.
Krakowski
, A. C., L. F.
Eichenfield
, and M. A.
Dohil
. "Management of Atopic Dermatitis in the Pediatric Population."
Pediatrics
122.4 (2008): 812-24. Web.