
V 3 Approved by Executive Committee of the Medical Staff on 10 19 2021 Perform clinical assessment to identify source and extent of infection Obtain Infectious Diseases ID consu ID: 937196
Download Pdf The PPT/PDF document "Department of Clinical Effectiveness" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



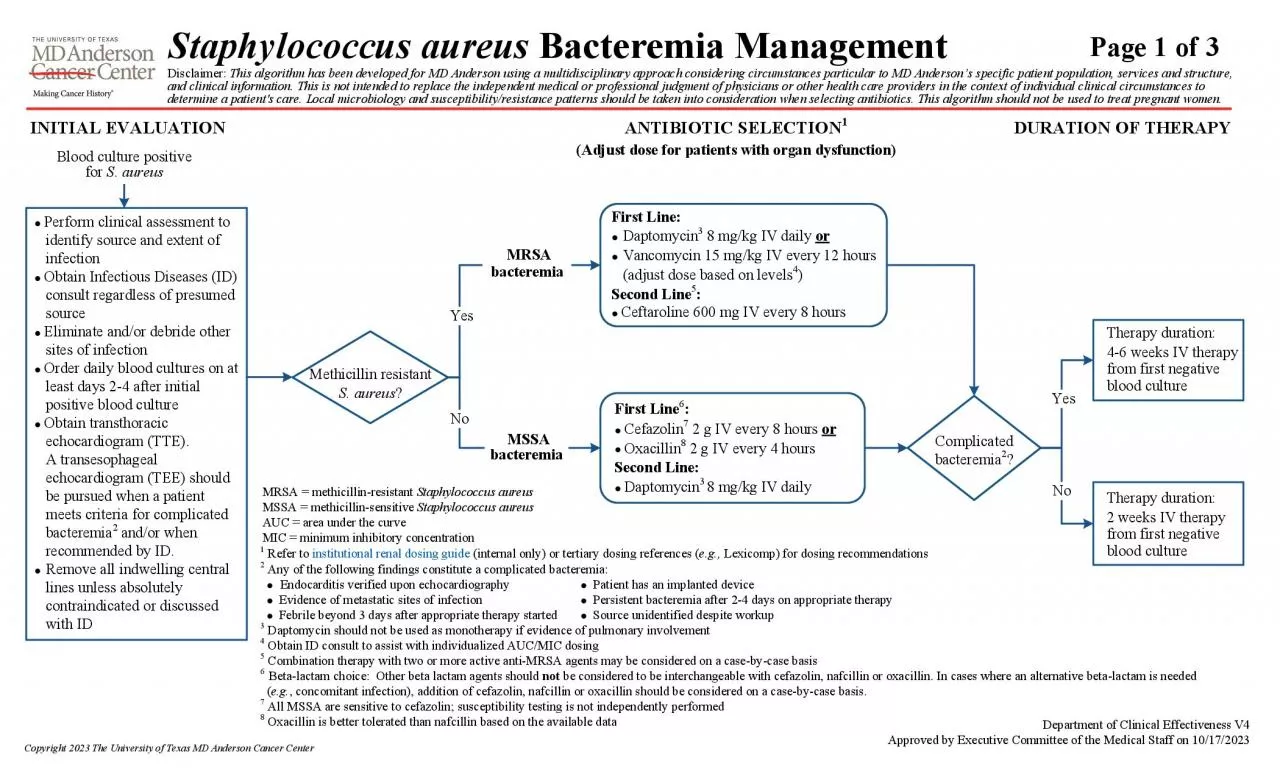
Department of Clinical Effectiveness V 3 Approved by Executive Committee of the Medical Staff on 10 / 19 / 2021 â Perform clinical assessment to identify source and extent of infection â Obtain Infectious Diseases ( ID ) consult regardless of colony count or presumed source â Eliminate and / or debride other sites of infection â Order daily blood cultures on at least days 2 - 4 after initial positive blood culture â Obtain transthoracic echocardiogram ( TTE ). A transesophageal echocardiogram ( TEE ) should be pursued when a patient meets criteria for complicated bacteremia 1 and / or when recommended by ID . â Remove all indwelling central lines unless absolutely contraindicated or discussed with ID First Line : â Daptomycin 2 , 3 8 mg / kg IV daily or â Vancomycin 2 15 mg / kg IV every 12 hours ( adjust dose based on levels ) Second Line 4 : â Ceftaroline 2 600 mg IV every 8 hours â Telavancin 2 7 . 5 mg / kg ( maximum 750 mg ) IV daily Methicillin resistant S . aureus ? MRSA bacteremia MSSA bacteremia Therapy duration : 4 - 6 weeks IV therapy from first negative blood culture Complicated bacteremia 1 ? Therapy duration : 2 weeks IV therapy from first negative blood culture Yes Yes No No 1 Any of the following findings constitute a complicated bacteremia : â Endocarditis verified upon echocardiography â Patient has an implanted device â Evidence of metastatic sites of infection â Persistent bacteremia after 2 - 4 days on appropriate therapy â Febrile beyond 3 days after appropriate therapy started â Source unidentified despite workup 2 Renal adjustment required as appropriate - refer to Antimicrobial Stewardship inside page for dosing recommendations : https :// mdandersonorg . sharepoint . com / sites / antimicrobial - stewardship 3 Daptomycin should not be used as monotherapy if evidence of pulmonary involvement 4 Combination therapy with two or more active anti - MRSA agents may be considered on a case - by - case basis 5 Beta - lactam choice : Other beta lactam agents should not be considered to be interchangeable with cefazolin , nafcillin or oxacillin . In cases where an alternative beta - lactam is needed ( e . g . , concomitant infection ) , addition of cefazolin , nafcillin or oxacillin should be considered on a case - by - case basis . 6 All MSSA are sensitive to cefazolin ; susceptibility testing is not independently performed 7 Oxacillin is better tolerated than nafcillin based on the available data First Line 5 : â Cefazolin 2 , 6 2 g IV every 8 hours or â Oxacillin 7 2 g IV every 4 hours Second Line : â Daptomycin 2 , 3 8 mg / kg IV daily INITIAL EVALUATION ANTIBIOTIC SELECTION Blood culture positive for S . aureus DURATION OF THERAPY MRSA = methicillin - resistant Staphylococcus aureus MSSA = methicillin - sensitive Staphylococcus aureus Page 1 of 4 Staphylococcus aureus Bacteremia Management Disclaimer : This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson â s specific patient population , services and structure , and clinical information . This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient ' s care . L ocal microbiology and susceptibility / resistance patterns should be taken into consideration when selecting antibiotics . This algorithm should not be used to treat pregnant women . SUGGESTED READINGS Buehrle , K . , Pisano , J . , Han , Z . , & Pettit , N . ( 2017 ). Guideline compliance and clinical outcomes among patients with staphylococcus aureus bacteremia with infectious diseases consultation in addition to antimicrobial stewardship - directed review . American Journal of Infec
tion Control , 45 ( 7 ) , 713 - 716 . doi : 10 . 1016 / j . ajic . 2017 . 02 . 030 Cheng , M . P . , Lawandi , A . , Butler - Laporte , G . , De l â Étoile - Morel , S . , Paquette , K . , & Lee , T . C . ( 2021 ). Adjunctive daptomycin in the treatment of methicillin - susceptible staphylococcus aureus bacteremia : A randomized , controlled trial . Clinical Infectious Diseases , 72 ( 9 ) , e 196 - e 203 . doi : 10 . 1093 / cid / ciaa 1000 Cosimi , R . A . , Beik , N . , Kubiak , D . W . , & Johnson , J . A . ( 2017 ). Ceftaroline for severe methicillin - resistant staphylococcus aureus infections : A systematic review . Open Forum Infectious Diseases , 4 ( 2 ) , ofx 084 . doi : 10 . 1093 / ofid / ofx 084 Geriak , M . , Haddad , F . , Rizvi , K . , Rose , W . , Kullar , R . , LaPlante , K . , ... Sakoulas , G . ( 2019 ). Clinical data on daptomycin plus ceftaroline versus standard of care monotherapy in the treatment of methicillin - resistant Staphylococcus aureus bacteremia . Antimicrobial Agents and Chemotherapy , 63 ( 5 ) , e 02483 - 18 . doi : 10 . 1128 / AAC . 02483 - 18 Goto , M . , Schweizer , M . L . , Vaughan - Sarrazin , M . S . , Perencevich , E . N . , Livorsi , D . J . , Diekema , D . J . , ⦠Ohl , M . E . ( 2017 ). Association of evidence - based care processes with mortality in staphylococcus aureus bacteremia at veterans health administration hospitals , 2003 - 2014 . JAMA Internal Medicine , 177 ( 10 ) , 1489 - 1497 . doi : 10 . 1001 / jamainternmed . 2017 . 3958 Grillo , S . , Cuervo , G . , Carratalà , J . , Grau , I . , Pallarès , N . , Tebé , C . , ... Pujol , M . ( 2019 ). Impact of β - lactam and daptomycin combination therapy on clinical outcomes in methicillin - susceptible staphylococcus aureus bacteremia : A propensity score â matched analysis . Clinical Infectious Diseases , 69 ( 9 ) , 1480 - 1488 . doi : 10 . 1093 / cid / ciz 018 Kullar , R . , Casapao , A . M . , Davis , S . L . , Levine , D . P . , Zhao , J . J . , Crank , C . W . , ⦠Rybak , M . J . ( 2013 ). A multicentre evaluation of the effectiveness and safety of high - dose daptomycin for the treatment of infective endocarditis . The Journal of Antimicrobial Chemotherapy , 68 ( 12 ) , 2921 - 2926 . doi : 10 . 1093 / jac / dkt 294 Li , J . , Echevarria , K . L . , & Traugott , K . A . ( 2017 ). β â Lactam therapy for Methicillin â Susceptible staphylococcus aureus bacteremia : A comparative review of cefazolin versus antistaphylococcal penicillins . Pharmacotherapy : The Journal of Human Pharmacology and Drug Therapy , 37 ( 3 ) , 346 - 360 . doi : 10 . 1002 / phar . 1892 Liu , C . , Bayer , A . , Cosgrove , S . E . , Daum , R . S . , Fridkin , S . K . , Gorwitz , R . J . , ⦠Chambers , H . F . ( 2011 ). Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin - resistant staphylococcus aureus infections in adults and children . Clinical Infectious Diseases , 52 ( 3 ) , e 18 - e 55 . doi : 10 . 1093 / cid / ciq 146 McDanel , J . S . , Perencevich , E . N . , Diekema , D . J . , Herwaldt , L . A . , Smith , T . C . , Chrischilles , E . A . , ⦠Schweizer , M . L . ( 2015 ). Comparative effectiveness of beta - lactams versus vancomycin for treatment of methicillin - susceptible staphylococcus aureus bloodstream infections among 122 hospitals . Clinical Infectious Diseases , 61 ( 3 ) , 361 - 367 . doi : 10 . 1093 / cid / civ 308 McDanel , J . S . , Roghmann , M . - C . , Perencevich , E . N . , Ohl , M . E . , Goto , M . , Livorsi , D . J . , ⦠Schweizer , M . L . ( 2017 ). Comparative effectiveness of cefazolin versus nafcillin or oxacillin for treatment of methicillin - susceptible staphylococcus aureus infections complicated by bacteremia : A nationwide cohort stu
dy . Clinical Infectious Diseases , 65 ( 1 ) , 100 - 106 . doi : 10 . 1093 / cid / cix 287 McCreary , E . K . , Kullar , R . , Geriak , M . , Zasowski , E . J . , Rizvi , K . , Schulz , L . T . , ⦠Rose , W . E . ( 2020 ). Multicenter cohort of patients with methicillin - resistant Staphylococcus aureus bacteremia receiving daptomycin plus ceftaroline compared with other MRSA treatments . Open Forum Infectious Diseases 7 ( 1 , ofz 538 ). doi : 10 . 1093 / ofid / ofz 538 Continued on next page Page 2 of 4 Staphylococcus aureus Bacteremia Management Disclaimer : This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson â s specific patient population , services and structure , and clinical information . This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient ' s care . L ocal microbiology and susceptibility / resistance patterns should be taken into consideration when selecting antibiotics . This algorithm should not be used to treat pregnant women . Department of Clinical Effectiveness V 3 Approved by Executive Committee of the Medical Staff on 10 / 19 / 2021 SUGGESTED READINGS - continued Neely , M . N . , Youn , G . , Jones , B . , Jelliffe , R . W . , Drusano , G . L . , Rodvold , K . A . , & Lodise , T . P . ( 2014 ). Are vancomycin trough concentrations adequate for optimal dosing ? Antimicrobial Agents and Chemotherapy , 58 ( 1 ) , 309 - 316 . doi : 10 . 1128 / AAC . 01653 - 13 Paul , M . , Zemer â Wassercug , N . , Talker , O . , Lishtzinsky , Y . , Lev , B . , Samra , Z . , ⦠Bishara , J . ( 2011 ). Are all beta â lactams similarly effective in the treatment of methicillin â sensitive staphylococcus aureus bacteraemia ? Clinical Microbiology and Infection , 17 ( 10 ) , 1581 - 1586 . doi : 10 . 1111 / j . 1469 - 0691 . 2010 . 03425 . x Paulsen , J . , Solligård , E . , Damås , J . K . , DeWan , A . , Åsvold , B . O . , & Bracken , M . B . ( 2016 ). The impact of infectious disease specialist consultation for staphylococcus aureus bloodstream infections : A systematic review . Open Forum Infectious Diseases , 3 ( 2 ) , ofw 048 . doi : 10 . 1093 / ofid / ofw 048 Prybylski , J . P . ( 2015 ). Vancomycin trough concentration as a predictor of clinical outcomes in patients with staphylococcus aureus bacteremia : A meta â analysis of observational studies . Pharmacotherapy : The Journal of Human Pharmacology and Drug Therapy , 35 ( 10 ) , 889 - 898 . doi : 10 . 1002 / phar . 1638 Rao , S . N . , Rhodes , N . J . , Lee , B . J , Scheetz , M . H . , Hanson , A . P . , Segreti , J . , ⦠Wang , S . K . ( 2015 ). Treatment outcomes with cefazolin versus oxacillin for deep - seated methicillin - susceptible staphylococcus aureus bloodstream infections . Antimicrobial Agents and Chemotherapy , 59 ( 9 ) , 5232 - 5238 . doi : 10 . 1128 / AAC . 04677 - 14 Schweizer , M . L . , Furuno , J . P . , Harris , A . D . , Johnson , J . K . , Shardell , M . D . , McGregor , J . C . , ⦠Perencevich , E . N . ( 2011 ). Comparative effectiveness of nafcillin or cefazolin versus vancomycin in methicillin - susceptible staphylococcus aureus bacteremia . BMC Infectious Diseases , 11 , 279 . doi : 10 . 1186 / 1471 - 2334 - 11 - 279 Schweizer , M . L . , Richardson , K . , Vaughan Sarrazin , M . S . , Goto , M . , Livorsi , D . J . , Nair , R . , ⦠Perencevich , E . N . ( 2021 ). Comparative effectiveness of switching to daptomycin versus remaining on vancomycin among patients with methicillin - resistant staphylococcus aureus ( MRSA ) bloodstream infections . Clinical Infectious Diseases , 72 ( Suppl 1 ) , 568 - 573 . doi : 10 . 1
093 / cid / ciaa 1572 Seaton , R . A . , Menichetti , F . , Dalekos , G . , Beiras - Fernandez , A . , Nacinovich , F . , Pathan , R . , & Hamed , K . ( 2015 ). Evaluation of effectiveness and safety of high - dose daptomycin : Results from patients included in the European Cubicin® Outcomes Registry and Experience . Advances in Therapy , 32 ( 12 ) , 1192 - 1205 . doi : 10 . 1007 / s 12325 - 015 - 0267 - 4 Timbrook , T . T . , McKay , L . , Sutton , J . D . , & Spivak , E . S . ( 2020 ). Disproportionality analysis of safety with nafcillin and oxacillin with the DFA Adverse Event Reporting System ( FAERS ). Antimicrobial Agents and Chemotherapy , 64 ( 3 ) , e 01818 - e 01819 . doi : 10 . 1128 / AAC . 01818 - 19 van Hal , S . J . , Paterson , D . L . , & Lodise , T . P . ( 2013 ). Systematic review and meta - analysis of vancomycin - induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter . Antimicrobial Agents and Chemotherapy , 57 ( 2 ) , 734 - 744 . doi : 10 . 1128 / AAC . 01568 - 12 Viehman , J . A . , Oleksiuk L . M . , Sheridan K . R . , Byers K . E . , He , P . , Falcione B . A . , & Shields R . K . ( 2016 ). Adverse events lead to drug discontinuation more commonly among patients who receive nafcillin than among those who receive oxacillin . Antimicrobial Agents and Chemotherapy , 60 ( 5 ) , 3090 - 3095 . doi : 10 . 1128 / AAC . 03122 - 15 Wilson , S . E . , Graham , D . R . , Wang , W . , Bruss , J . B . , & Castaneda - Ruiz , B . ( 2017 ). Telavancin in the treatment of concurrent staphylococcus aureus bacteremia : A retrospective analysis of ATLAS and ATTAIN studies . Infectious Diseases and Therapy , 6 ( 3 ) , 413 - 422 . doi : 10 . 1007 / s 40121 - 017 - 0162 - 1 Page 3 of 4 Staphylococcus aureus Bacteremia Management Disclaimer : This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson â s specific patient population , services and structure , and clinical information . This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient ' s care . L ocal microbiology and susceptibility / resistance patterns should be taken into consideration when selecting antibiotics . This algorithm should not be used to treat pregnant women . Department of Clinical Effectiveness V 3 Approved by Executive Committee of the Medical Staff on 10 / 19 / 2021 This practice consensus statement is based on majority opinion of the Staphylococcus aureus Bacteremia Management workgroup at the University of Texas MD Anderson Cancer Center for the patient population . Theses experts included : DEVELOPMENT CREDITS Ŧ Core Development Lead ⦠Clinical Effectiveness Development Team Antimicrobial Stewardship Team Ŧ Javier Adachi , MD ( Infectious Disease ) Olga N . Fleckenstein , BS ⦠Thoa Kazantsev , MSN , RN , OCN ⦠Samuel Shelburne , MD , PhD ( Infectious Diseases ) Page 4 of 4 Staphylococcus aureus Bacteremia Management Disclaimer : This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson â s specific patient population , services and structure , and clinical information . This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient ' s care . L ocal microbiology and susceptibility / resistance patterns should be taken into consideration when selecting antibiotics . This algorithm should not be used to treat pregnant women . Department of Clinical Effectiveness V 3 Approved by Executive Committee of the Medical Staff on 10 / 19 / 202