
Dr Ayisha Qureshi Assistant Professor MBBS Mphil THE REPRODUCTIVE SYSTEM The reproductive system does NOT contribute to HOMEOSTASIS and is NOT essential for survival of an individual ID: 776631
Download Presentation The PPT/PDF document " FEMALE REPRODUCTIVE SYSTEM" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

Slide1
FEMALE REPRODUCTIVE SYSTEM
Dr.
Ayisha
Qureshi
Assistant Professor
MBBS,
Mphil
Slide2THEREPRODUCTIVE SYSTEM
The reproductive system does NOT contribute to HOMEOSTASIS and is NOT essential for survival of an individual.
Slide3Functions of the Female Reproductive System
Slide4SEXUAL LIFE OF A FEMALE
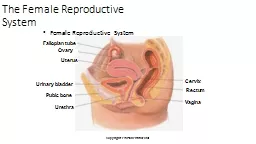
Slide5Parts of Female Reproductive System
Slide6OVARIES
It is the gonad or the primary sex organ in the Female. A woman has 2 ovaries. An ovary performs 2 functions:Gametogenesis (OOGENESIS): leads to the production & release of ovum or egg (the female gamete). Endocrine Function: secretion of female sex hormones (ESTROGENS & PROGESTERONE).
Slide7STRUCTURE OF THE OVARY:
Ovaries are flattened ovoid bodies, with the dimensions of4 x 2 x 1 cm. Each ovary is attached at the hilum to the broad ligament, by means of mesovarium and ovarian ligament. Each ovary has 2 portions: 1. CORTEX: is the outer portion & is lined by the germinal epithelium underneath a fibrous layer known as Tunica Albuginea. It consists of ovarian follicles at different stages, connective tissue & Interstitium. 2. MEDULLA: is the inner portion & contains blood vessels, lymphatics, nerve fibers and smooth muscle fibers near the hilum.
Slide8OVARY IN THE INTRAUTERINE LIFE
PRIMORDIAL GERM CELLS
(the most primitive germ cells)
3
rd
Week of Gestation
↓
OOGONIA
(the female germ cell)
6
th
Week of Gestation
Undergoes Mitosis
↓
PRIMARY OOCYTE
8
th
week of gestation till BIRTH
Completes Mitosis . Meiosis starts & gets arrested at the
Diplotene
stage.
Meiosis stays in the arrested stage until a Primary Oocyte becomes destined for Ovulation
at/after Puberty
↓
Primordial Follicle containing the Primary oocyte
(The primary oocyte becomes surrounded by a single layer of flattened
granulosa
cells)
MITOSIS + MEIOSIS + ATRESIA
6-7 million
oogonia
at 20
th
week of gestation are reduced to only 1-2 million Primary Oocytes at BIRTH
Slide9In the Intrauterine life, the germ cell (the undifferentiated gonad cell) forms the OOGONIA in the females. It then completes the mitotic replication and Meiosis by 5th month of fetal development at which point it is called the Primary Oocyte . The Primary Oocyte is actually the egg arrested in the Prophase of the Meiosis and its follicular development shows a single layer of zona granulosa around the oocyte , thus it is also called the Primordial Follicle. The Primary Oocyte remains arrested in this phase from birth to the time of its ovulation which comes after puberty has been reached….
Slide10The menstrual cycle
Slide11THE MENSTRUAL CYCLE
Definition:
Menstrual cycle is defined as cyclic events that take place in a rhythmic fashion during the reproductive period of a female’s life.
Menstrual cycle starts with Menarche which also marks the onset of puberty.
Duration:
U
sually 28 days (may vary b/w 20 & 40 days).
Slide12THE MENSTRUAL CYCLE
Slide13CHANGES DURING MENSTRUAL CYCLE
During each menstrual cycle, series of changes occur in the ovaries & the accessory sex organs. These changes are divided into 4 groups:
Ovarian Changes
Uterine Changes
Vaginal Changes
Changes in the Cervix
Slide14OVARIAN CHANGES
Slide15OVARIAN CHANGES
After the onset of puberty, the ovary alternates b/w 2 phases:
1. Follicular Phase: (Day 1-14)
- characterized by presence of maturing follicles.
- the recruitment & development of primordial ovarian follicles starts during menstruation.
2. Luteal Phase: (Day 15-28)
- starts with ovulation and formation of the corpus
luteum
.
- the luteinized
granulosa
cells start producing progesterone.
Normally, this cycle is interrupted only by pregnancy and terminates with menopause.
Slide16Slide17FOLLICULAR PHASE OF THE OVARIAN CYCLE:
It extends from Day 1 to day 14 of the Menstrual cycle. At Day 14, Ovulation takes place. During this phase, a few primordial follicles start growing but only 1 reaches maturity and is released during ovulation as the Mature ovum.
Slide18PRIMORDIAL FOLLICLE
Ovum surrounded incompletely by the
granulosa
cells. These cells provide nutrition to the ovum during the childhood & also secrete the oocyte maturation inhibiting factor which keeps the ovum in the immature stage from birth till puberty.
↓
At the onset of puberty, with each menstrual cycle, under influence of FSH, about 6-12 primordial follicles start developing into the Primary Follicles. This is called
Recruitment of Primary Follicles.
↓
PRIMARY FOLLICLE
Ovum is completely surrounded by the
granulosa
cells.
Increase in size of the ovum.
Onset of formation of connective tissue capsule around the follicle called the
Theca cells
.
↓
VESICULAR FOLLICLE / ANTRAL FOLLICLE/ SECONDARY FOLLICLE
Slide19VESICULAR FOLLICLE / ANTRAL FOLLICLE/ SECONDARY FOLLICLE
Accelerated proliferation
of
granulosa
cells giving rise to many more layers of cells.
These cells develop
receptors
for
FSH, increasing their sensitivity to FSH
which brings about more
proliferation
of the follicles.
Granulosa
cells secrete liquor
folliculi
into a
cavity
between the
granulosa
cells called
the
follicular cavity or
antrum
. This liquid has a high concentration of
Estrogen.
Ovum increases in size and is pushed to one side and is surrounded by the
granulosa
cells called the
cumulus
oophorus
or germ hill.
A thick, glycoprotein
membrane
is secreted by the
granulosa
cells around
the ovum
and is called
zona
pellucida
.
Theca cells differentiate into:
T
heca
interna
:
which becomes secretory in nature & starts secreting Estrogens & Progesterone.
Theca
externa
:
forms the capsule of the developing follicle.
(
Thecal
cells synthesize androgens that diffuse into the neighboring
granulosa
cells, where the enzyme aromatase converts them to estrogens.)
↓
GRAAFIAN FOLLICLE/ MATURE OVARIAN FOLLICLE
About 7 days later
.
One follicle outgrows all others; the remaining 5-11 involute, a process called atresia. These follicles are said to become
atretic
.
The oocyte completes Meiosis I and forms the Secondary Oocyte &
F
irst
P
olar body. Secondary Oocyte starts Meiosis II & is arrested in the Metaphase. It will only progress if fertilized.
↓
OVULATION
Slide20Slide21OVULATION
Definition:
It is the process by which the
Graafian
Follicle ruptures with consequent discharge of ovum into the abdominal cavity. It is under influence of LH. Ovulation occurs on the 14
th
day of menstrual cycle in a 28 day cycle. The ovum enters the Fallopian tube.
Process:
Rupture of
Graafian
Follicle at the
stigma
(small area in the middle of the follicular capsule that swells rapidly & protrudes like a nipple).
Follicular fluid oozes out.
Ovum expelled into the abdominal cavity
(Ovum+ Corona
radiata
)
.
From there it enters the Fallopian tube through the
fimbriated
end.
The ovum is viable only for 24-48 hours. So it must be fertilized within that time.
Slide22ROLE OF LH IN OVULATION: LH SURGE
The increase in LH concentrations just before ovulation is called the
LH Surge
and is
necessary for Ovulation. Without this hormone, even when large quantities of FSH are available, there will be no ovulation.
This is because:
About 2 days before ovulation, LH secretion by the anterior pituitary gland increases 6 to 10-fold and peaks about 16 hours before ovulation.
LH
& FSH synergistically cause rapid
swelling of the follicle during the last few days before ovulation.
LH converts the theca cells into progesterone-secreting cells, thus, the rate of secretion of estrogen falls 1 day before ovulation.
Under these effects, 2 things happen:
Theca
externa
begins to release
proteolytic
enzymes (esp. collagenase) that dissolve the follicular capsule wall leading to degeneration of the stigma.
Secretion of Prostaglandins into the follicular tissue which leads to the smooth muscle contraction of the follicle leading to expulsion of the ova.
This leads to degeneration of the stigma and discharge of the ovum.
Slide23Slide24Role of the LH Surge
1.
It halts estrogen synthesis by the follicular
cells.
2.
It reinitiates meiosis in the oocyte of the developing
follicle by
blocking release of an
oocyte maturation–inhibiting
substance
produced
by the
granulosa
cells.
This
substance is
responsible for
arresting meiosis in the primary oocytes once they
are wrapped
within
granulosa
cells in the fetal ovary.
3.
It triggers production of local prostaglandins, which
induce ovulation
by promoting vascular changes that cause rapid
follicular swelling
while inducing enzymatic digestion of the
follicular wall
. Together these actions lead to rupture of the
weakened wall
that covers the bulging
follicle.
4.
It causes
differentiation
of follicular cells into luteal
cells. Because
the LH surge triggers both ovulation and
luteinization
, formation
of the corpus
luteum
automatically follows
ovulation. Thus
, the
midcycle
burst in LH secretion is a
dramatic point
in the cycle; it terminates the follicular phase
and initiates
the luteal
phase.
Slide25Slide26LUTEAL PHASE:
It extends between 15
th
and 28
th
day of the menstrual cycle. During this phase Corpus
luteum
is developed & thus it is called luteal phase.
Slide27CORPUS LUTEUM
Corpus luteum is the glandular yellow structure developed from the ruptured Graafian follicle after the release of the ovum. It is also called yellow body. Ovulation ↓Corpus Hemorrhagicum (follicle is filled with blood which clots slowly)↓Corpus Luteum (granulosa & theca interna cells are transformed into lutien cells & secrete Progesterone)If fertilization occurs: Corpus luteum of PregnancyIf no fertilization: Corpus albicans (white scar tissue)
Slide28Functions of Corpus Luteum
1. Secretion of hormones:
It acts as a temporary endocrine gland. Secretes large
quantities of Progesterone & small quantities of Estrogens. LH influences the secretion of these 2 hormones.
2. Maintenance of Pregnancy:
If pregnancy occurs, corpus
luteum
remains active for 3 months and maintains the pregnancy by secreting various hormones. The pregnancy cannot survive if corpus
luteum
is removed in the early weeks of pregnancy. i.e. before placenta starts secreting the same hormones.
Slide29Primordial Follicle
↓Primary Follicle (Primary Oocyte)↓Secondary Follicle ↓Vesicular Follicle ↓Graafian Follicle (Secondary Oocyte)(Growth takes place under the influence of FSH) ↓OVULATION(Takes place under the influence of LH)↓Corpus Hemorrhagicum (follicle is filled with blood which clots slowly)↓Corpus Luteum (granulosa & theca interna cells are transformed into lutien cells )
FOLLICULAR PHASE
LUTEAL PHASE
Slide30APPLIED ANATOMY OF OVULATION
Why is it significant to determine the Ovulation time?
Determination of time of Ovulation is significant for:
- Family Planning by rhythm method.
- Encouraging fertility in couples trying to conceive.
How is the ovulation time determined?
Various indirect methods are available to determine the ovulation time:
1. Determination of Basal body temperature:
There is an increase in the temperature of 0.3-0.5° C due to
thermogenic
effect of Progesterone. A temperature chart plotted during the month can indicate the time of ovulation.
2. Determination of Hormonal levels in Plasma:
Plasma levels of FSH, LH, Estrogen & Progesterone is measured. Hormone level is altered at the time of ovulation.
3. Ultrasound Scanning:
Process of ovulation can be observed during ultrasound scanning.
Slide31Uterine changes
Slide32UTERINE CHANGES
During each menstrual cycle, along with ovarian changes, the uterus also undergoes changes simultaneously. Average blood lost during a menstrual cycle is 30-50 ml. They occur in 3 phases:
Menstrual Phase
Proliferative Phase
Secretory Phase
Slide33The Menstrual Cycle
Slide34Slide35Menstrual Blood Flow: POINTS TO NOTE
The volume of the blood loss during the menstrual phase is about 30-50 ml. More than 80 ml is considered pathological and is termed
menorrhagia.
Bleeding continues for 3-7 days (average 4 days).
Most of the blood lost (75%) is arterial blood.
The menstrual blood flow is not clotted because of the
Fibrinolysin
acting on the blood in the uterine cavity and because it has clotted previously and therefore, it lacks fibrinogen.
Presence of clots signifies excess, pathological blood loss.
The uterine myometrium (muscle) shows strong contractions that expel the contents of the uterine cavity. If very strong these contractions can cause pain during menstruation called
Dysmenorrhea.
Slide36Slide37Slide38Slide39HORMONES & THEIR ROLE IN MENSTRUAL CYCLE
Hypothalamus: releases GnRH. Anterior Pituitary: releases FSH & LH. Ovarian Hormones: Estrogens & Progesterone
Slide40APPLIED PHYSIOLOGY
AMENORRHEA:
Absence of menstruation
HYPOMENORRHEA:
Decreased
m
enstrual bleeding.
MENORRHAGIA:
Excess menstrual bleeding.
OLIGOMENORRHEA
: Decreased frequency of menstrual bleeding.
DYSMENORRHEA:
Menstruation with pain.
Slide41HORMONES SYNTHESIZED BY THE OVARY
Slide42The following hormones are produced by the ovary:
Steroid Hormones:
- Estrogens
- Androgens
- Progesterone
2. Peptide Hormones:
-
Inhibin
A:
from
granulosa
and theca cells of the corpus
luteum
. Has a negative feedback effect on FSH but has little importance.
-
Inhibin
B:
from
granulosa
cells. Has a negative feedback effect on FSH secretion that is more potent than
Inhibin
A.
-
Activin
:
stimulates the FSH secretion.
-
Folliculostatin
:
inhibits the FSH secretion by binding and inactivating
Activin
.
-
Anti-
Mullerian
hormone:
from the
granulosa
cells. It inhibits the recruitment of primordial follicles into the follicular pool by inhibiting aromatase production.
Slide43estrogen
The main function of estrogen is to proliferate and promote the growth of specific cells in the body that are responsible for the development of most secondary sexual characteristics of the female.
Slide44ESTROGENS
Source
: Estrogens are secreted in large quantities by the theca
interna
cells of the ovaries
&
the corpus
luteum
& to
a
smaller
amount by
the
placenta and adrenal cortex.
Estrogen is derived from androgens, esp.
androstendione
, which
are
secreted in large amounts
in the theca
interna
cells.
Androgens
migrate
from theca cells to the
granulosa
cells, where it is converted into estrogen by the activity of the aromatase
enzyme (theca cells do not have the enzyme aromatase).
Chemistry
: It is a steroid.
Different forms:
-
β
- Estradiol or Estradiol (the most potent estrogen)
-
E
strone
-
Estriol
(the least potent estrogen)
Half-life:
30-60 minutes
Transport:
Only 2% is free; while 98% is bound with plasma proteins. mostly by albumin & to a lesser extent by the globulin called as
sex hormone binding globulin (SHBG).
Slide45Slide46Slide47Functions of Estrogens:
Effect on Ovarian Follicles:
Stimulatory
Effect on Uterus:
prepares the uterus for pregnancy thru the following changes:
- enlargement of uterus.
- increased blood supply to endometrium.
- Proliferation & dilatation of blood vessels & endometrial glands.
3.
Effect on Fallopian tubes:
S
timulatory aiding in the fertilization process in the fallopian tubes.
4.
Effect on Vagina:
stimulatory thus preventing certain common vaginal infections.
5.
Feminizing Effects & Puberty:
- Secondary
Sexual
characteristics:
1. Hair distribution
2. Skin: smooth & increased vascularity.
3. Body shape becomes feminine.
4. Pelvis: broadening of pelvis with increased transverse diameter.
5. Voice: high-pitched voice.
6.
Effect
on Breasts:
aids in breast development preparing the
breast
for lactation. However, at birth
due
to
expulsion
of placenta, it leads to a decrease in estrogen
levels
and prolactin
secretion
starts. Administration of
large
amounts of estrogen prevents lactation as it has
an
anti-prolactin action.
Slide487
.
Effect on Bones:
Stimulates
Osteoblastic
activities. Because
of
decreased amounts of estrogen after
menopause
,
it
leads to Osteoporosis in old age.
8.
Effect on Metabolism:
- anabolism in proteins increasing total body proteins.
- deposition of fat in the female body.
9.
Effect on Electrolyte balance:
causes sodium & water
retention
. This effect becomes more
pronounced
in
pregnancy
.
10.
Effects on Gonadotropin secretion:
Estrogen decreases the secretion of FSH and LH by inhibiting the secretion of
GnRH
of the hypothalamus as well as by a direct inhibitory effect on the
adenohypophysis
.
11.
Effect on Blood Pressure:
It increases the production of angiotensinogen in the liver leading to an increase in Blood pressure. This effect is likely to occur in women using contraceptives containing an estrogen.
12.
Effects on blood clotting:
It leads to an increase in the formation of blood clotting factors while causing a decrease in anti-thrombin III levels. These effects lead to blood clotting. In women on estrogen contraceptives, venous thrombosis can occur.
13
. Carcinogenesis:
In women, treatment with estrogen has been shown to increase the incidence of breast cancer.
Slide49REGULATION OF ESTROGEN SECRETION
Slide50progesterone:
The main function of the
Progestins
is to prepare the uterus for pregnancy & the breasts for lactation.
Slide51Progesterone
Source:
a small amount by the theca
interna
cells of the ovaries & a larger amount by the corpus
luteum
. A small amount is also secreted by the adrenal cortex and the placenta.
In the follicular phase, theca
interna
cells produce
pregnenolone
& progesterone,
that enters the
granulosa
cells
where most of it is converted into estrogen. However, in
the luteal phase,
the theca cells of the
corpus
luteum
secretes
much larger
amounts of
Progesterone so that even after most of it is converted into estrogen there is still a lot of Progesterone that is secreted.
Other names:
-
Progestins
.
-
Progestagens
.
-
Gestagens
.
Chemistry:
s
teroid.
Half-life:
4-5 minutes
Transport:
About 2% is transported in the free form while 98% is transported in the bound form. It is found bound to albumin & Cortisol binding globulin (CBG).
Slide52Slide53FUNCTIONS OF PROGESTERONE:
1. Effect on Fallopian tubes:
secretory activities are increased for nutrition of the fertilized ovum.
2. Effect on Endometrium of Uterus:
promotes secretory activities of the endometrium to prepare the uterus for the implantation of the fertilized ovum.
3. Effect on Myometrium of Uterus:
It causes anti-estrogenic effect on the myometrium of uterus by decreasing estrogen receptors on it. This leads to the myometrium becoming less responsive to the excitatory effects of estrogen. Same effect is seen for oxytocin. This decreases the spontaneous rhythmic contractions of the uterus, and helps in the maintenance of pregnancy.
4. Effect on Cervix:
increases the thickness of cervical mucosa inhibiting transport of sperm into uterus. This effect is used in the contraceptive
minipills
.
5. Effect on mammary glands:
increases the secretory function of the
breasts preparing them for lactation.
Slide54FUNCTIONS OF PROGESTERONE (cont.)
6. Effects on
Adenohypophysis
:
The progesterone secreted during the luteal phase of menstrual cycle and during pregnancy results in an inhibition of the secretion of FSH and LH. These effects result in a non-development of ovarian follicle and lack of ovulation and menstruation. Many contraceptive drugs contain progestin.
6. Thermogenesis:
This is shown by the raised body temperature (about 1°F) during the second half of the menstrual cycle. i.e. luteal or secretory phase. This is brought about by resetting of the thermoregulatory center of the hypothalamus at a higher level.
7. Effect on Respiration:
It stimulates respiration during luteal phase and pregnancy.
8. Competition with Aldosterone:
Progesterone competes with Aldosterone for occupying the latter’s receptors in the distal renal tubular cells. Thus, it prevents the action of Aldosterone and results in excess sodium and water loss. However, there is increased aldosterone secretion and condition is normalized. If aldosterone is absent then it leads to the same effects as aldosterone, although, the action is very weak.
8. Effects on Brain:
It has a depressant effect on the brain.
Slide55Puberty
The Period during which adolescents reach sexual maturity and become capable of reproduction.
Slide56Slide57Menopause
The cessation of a woman’s menstrual cycle between the ages of 45 and 55 is called Menopause.
Slide58MENOPAUSE
Menopause is partly attributed to the limited supply of ovarian follicles present at birth. Once this reservoir is depleted, ovarian cycle and hence menstrual cycle, ceases. More significantly, change in secretion by hypothalamus (GnRH) triggers the onset of menopause. The Menopause is characterized by: Increasingly irregular cycles.Decreasing estrogen levels. (Ovarian estrogen levels decrease from 300mg /day to nothing. )The loss of high levels of estrogen brings about many physical and emotional changes.
Slide59Post-Menopausal Hormone Therapy
Hormone Replacement Therapy (HRT): Estrogen alone or with a progestin is used to treat post-menopausal patients. The risks are endometrial cancer, venous thromboembolism and gall bladder disease.
Slide60Why males do not experience complete gonadal failure as females do and do not have menopause?
Slide61Fertilization
Slide62Slide63Slide64Slide65Pregnancy/ gestation
Slide66Body changes in Pregnancy
The body undergoes many physiological changes in various body systems during pregnancy. They are described as below:
Amenorrhea:
means the stoppage of menstruation. The increased plasma levels of estrogen and progesterone supplied first by the corpus
luteum
& later by the placenta inhibit the secretion of pituitary gonadotropins & lead to non-ovulation and amenorrhea throughout the pregnancy.
Uterus:
the non-pregnant uterus measures 7.5 x 5 x 2.5 cm & contains a potential cavity. It greatly enlarges during pregnancy. Estrogen contributes to the growth of the uterus but
s
tretch appears to be the major stimulus for the uterine growth .
Cervix:
enlarges and becomes soft in consistency (due to increased vascularity) in the pregnant woman as compared to being hard in the non-pregnant women. A firm plug of mucus is formed within the cervical canal which protects the pregnant uterus from any possibility of infection ascending from the vagina.
Slide67Body Changes in Pregnancy(cont.)
4. Blood: There is an increased plasma volume as well as an increased total RBC volume. But the plasma volume increases to a much greater extent than the red cell volume, so there is a fall in the blood Hb level. This anemia is due to hemodilution as well as due to iron deficiency (Iron therapy greatly decreases it). ESR is raised. There is Leukocytosis. There is hypercoagubility of the blood which is a beneficial effect against excessive bleeding during childbirth. But it also increases the risk of thromboembolic phenomena.
5. CVS:
The heart rate & the cardiac output both increase but the arterial blood pressure does not rise. Due to pressure of the enlarged uterus on the Inferior Vena Cava (IVC), pressure rises in the veins of the lower limbs & the lower part of the IVC. Varicose veins may be seen in the legs.
6. GIT:
The stomach & small intestines show a decreased motility. The colon shows sluggishness and constipation is common.
7. Nausea & Vomiting:
These are seen in early pregnancy, esp. in the morning (morning sickness). Occasionally, the vomiting may be very severe called as
Hyperemesis
Gravidarum
.
Slide68Body Changes in Pregnancy(cont.)
8. Respiration: The pulmonary ventilation is increased as Oxygen has to be supplied to the fetus as well. 9. Body weight: There is a gain of about 25-30 pounds body weight due to:Fetal mass (8 lbs)Amniotic fluid, Placenta (4 lbs)Increased size of uterus. (3 lbs)Increased body fat, protein and water. (15-20 lbs)10. Metabolic Changes: BMR is raised by about 15% due to the extra heat production by the fetus & the increased production of some hormones.Diabetes mellitus may appear in a woman during pregnancy known as Gestational Diabetes. Serum lipids are also raised.
11. Endocrinological changes:
The following changes take place:
As there is increased secretion of estrogen and Progesterone, LH & FSH secretion is suppressed.
Prolactin is secreted.
The formation of glucocorticoids & aldosterone is increased.
The pituitary GH secretion is suppressed due to action of
hCS
.
12. Excretory System:
The GFR & renal Plasma flow increases by about 50%; there is increased urine formation.
Slide69contraception
The deliberate use of artificial methods or other techniques to prevent pregnancy as a consequence of sexual intercourse.
Slide70Some methods of Contraception
Oral Contraceptives/ Birth Control Pills
IUD (Intrauterine Device)
Slide71Natural Contraception in Nursing Mothers
Women who nurse their infants do not have menstrual cycle for about 24-30 weeks after delivery. This is because regular nursing stimulates prolactin secretion and prolactin secretion inhibits
GnRH
secretion resulting in suppression of Gonadotropin secretion. In the absence of Gonadotropins (FSH & LH), the ovaries become inactive and ovulation does not occur.
Slide72Functions of placenta
Slide73PLACENTA
Placenta is a temporary membranous vascular organ that develops in females during pregnancy and is expelled after childbirth. Placenta forms a link between mother and fetus.
It is connected to the fetus by the umbilical cord which contains blood vessels and connective tissue.
It performs many functions. These functions are grouped under 2 main headings:
Endocrine functions of Placenta
Non-endocrine functions of Placenta
Slide74PLACENTA
Endocrine Functions
Secretion of the following hormones: Human chorionic gonadotropin (hCG)Estrogen: causes enlargement of uterus and development of the duct system of the breast. Progesterone: decreases the excitability of the uterus so that the fetus is not expelled. Also stimulates the growth of the fetus. Human chorionic somatomammotropin (hCS) Plasma parathyroid hormone related peptide (PTHrp): It increases maternal Ca levels to be used for the calcifying fetal bones. Miscellaneous hormones: such as ADH, ACTH, CRH, alpha-MSH, GnRH, inhibin, prolactin and androgens.
Non-endocrine Functions
Respiration:
Fetal lungs are non-functioning & placenta forms the respiratory organ.
Nutrition:
diffusion of electrolytes & hormones from mother’s blood into fetus through placenta.
Excretion:
metabolic end products from the fetal blood are excreted into the mother’s blood thru placenta.
Formation of
enzymes
Transfer of non-nutritional substances:
several bacteria, viruses & chemical can cross the placental barrier & enter the fetus from the mother’s blood.
M
aternal diseases like rubella, typhoid & syphilis can be transmitted to fetus. Drugs &
teratogenic
substances can also cross over into the fetal circulation.
Slide75PLACENTAL HORMONES
Human Chorionic Gonadotrophin (hCG)
It is a glycoprotein. Action on Corpus Luteum: Because of its LH-like action this hormone supports the secretory activity of the corpus luteum, which is the secretion of estrogen & progesterone, in the early months. These 2 hormones are essential for the maintenance of pregnancy. Later on placenta starts producing these 2 hormones itself. Action on developing Testis of the fetus: It stimulates the Leydig cells to increase their testosterone secretion.
Human Chorionic Somatomammotropin (hCS)
It is a protein. It is also called human placental
lactogen
.
It has activities of both Growth hormone & prolactin.
It causes decreased utilization of glucose by the mother making more glucose available for the fetus. This can also contribute to increased severity of Diabetes in pregnancy.
It helps in the conservation of proteins, potassium and calcium for use by the fetus.
It also causes lipolysis making large amounts of free fatty acids available as source of energy for the use by the mother.
Slide76Slide77During pregnancy,
three
endocrine
systems interact to support and enhance the growth and
development of the fetus, to coordinate the timing of parturition,
and to prepare the mammary glands for nourishing the
baby
after
birth:
placental hormones
maternal hormones and
fetal
hormones.
Slide78parturition
Childbirth/
Or
The act of giving birth to the young.
Slide79In females, pregnancy lasts for 40 weeks from the first day of the last menstruation. At the end of this term, the fetus is expelled from the female body through the process of parturition.
The stimulus which initiates the events resulting in delivery can be several factors, some of which are:
Oxytocin
Prostaglandins
A powerful positive feedback system is established by which contractions of the uterus become progressively more frequent and more powerful.
Slide80Oxytocin
causes the contraction of the uterus. Stretch of the uterine musculature. Stretch of the cervix.
Slide81lactation
Lactation means the synthesis, secretion and ejection of milk.
Slide82Estrogen stimulates growth of the ductal system of the breasts.
Progesterone is required for the development of the milk-secreting organ.
Prolactin
promotes
lactation:
Although estrogen and progesterone are essential for the physical development of the breasts during pregnancy, a specific effect of both these hormones is to
inhibit
the actual secretion of milk.
Conversely, the hormone
prolactin
has exactly the opposite effect on milk secretion-promoting it. This hormone is secreted by the mother's anterior pituitary gland, and its concentration in her blood rises steadily from the fifth week of pregnancy until birth of the baby, at which time it has risen to 10 to 20 times the normal
non-pregnant level.
4. Ejection
(or "Let-Down") Process
(discharge of milk from mammary gland)
is a function
of
Oxytocin.
Slide83