
Viet Nguyen MD Maria Valencia MD Achint Singh MD Wilson Altmeyer MD Carlos Bazan III MD Bundhit Tantiwongkosi MD eEdE155a Disclosure Statement The authors have no financial interest to disclose ID: 169546
Download Presentation The PPT/PDF document "Pictorial Review of Orbital Tumors and T..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

Slide1
Pictorial Review of Orbital Tumors and Tumor-like Lesions
Viet Nguyen, MDMaria Valencia, MDAchint Singh, MDWilson Altmeyer, MDCarlos Bazan III, MDBundhit Tantiwongkosi, MD
eEdE-155aSlide2
Disclosure Statement
The authors have no financial interest to disclose.Slide3
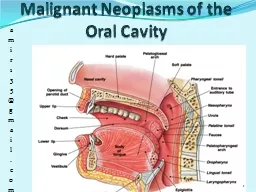
ObjectivesReview basic anatomy of the orbit
Illustrate characteristic imaging findings of orbital tumor and tumor-like lesions with respect to orbital compartmentsSlide4
Table of Contents
Introduction / AnatomyClick to proceed directly to section of choice.
Globe
Intraconal
Extraconal
Conal
Summary
MulticompartmentSlide5
IntroductionOrbital tumors and tumor-like lesions have a spectrum of imaging findings with
distinct outcome and treatment planningCompartmental approach of orbital lesions helps guide diagnostic considerationCT and MR play crucial role in diagnosis, treatment planning, follow up and surveillanceSlide6
Anatomy
Superior Oblique
Inferior Oblique
Superior Rectus
Inferior Rectus
Medial Rectus
Lateral Rectus
Optic Nerve
Ophthalmic Artery
Superior Ophthalmic Vein
Lacrimal Gland
Superior Orbital Fissure
Optic Canal
Levator
Palpebrae
Superioris
Conal
Intraconal
Globe
Extraconal
Click to highlight structure.Slide7
Anatomic Considerations
Orbital ForaminaContentsSuperior Orbital Fissure
Cranial nerve III, IV, V1, VISuperior ophthalmic veinMiddle meningeal artery, orbital branchSympathetic fibers
Optic Canal
Optic nerve
Ophthalmic artery
Sympathetic fibers
Infraorbital
Canal
Cranial
nerve V2
Infraorbital
artery & vein
Adapted from: Som
, Peter M., and Hugh D. Curtin. "Normal Orbital Anatomy." Head and Neck Imaging. St. Louis, MO: Mosby, 2011. 549-51.
http://commons.wikimedia.org/wiki/File:713_Bones_Forming_Orbit.jpg
http://commons.wikimedia.org/wiki/File:Schematic_diagram_of_the_human_eye_en.svgSlide8
Ocular Melanoma
S
agittal oblique MR images show
an avidly enhancing
,
high T1
/
low T2
signal
mass
in the posterior globe
extending to the adjacent sclera
& causing
partial retinal detachment (no enhancement)
.
E
nhancing
choroidal
mass with increased T1W MR signal; most common primary ocular tumor adult
Enhancement on MR distinguishes tumor from commonly associated retinal detachmentSlide9
Choroidal Melanoma
Coronal post contrast T1W MR image reveals
a focal linear area of enhancement
at the superior nasal aspect of the right globe, within the choroid layer. This was proven to be
choroidal
melanoma on histology. The tumor can be subtle in this case; therefore, correlation between imaging &
fundoscopic
findings are crucial.Slide10
Nodular Scleritis
Coronal & sagittal MR images of the orbits show an anterior right scleral lesion with
intermediate T1
/
low T2
signal intensity &
contrast enhancement
. This was a case of nodular
scleritis
mimicking a neoplasm in a patient with juvenile rheumatoid
arhritis
.
Thickening & enhancement
of the left
globe also represent
scleritis
. Slide11
Intraconal Orbital Hemangioma
MR imaging of the orbits reveals a well-defined, round
intraconal
mass displacing the optic nerve. The lesion shows
low T1,
high T2
signal intensity &
characteristic patchy enhancement
.
Well-defined, ovoid, enhancing mass with
patchy
enhancement
Most common adult orbital mass, typically
intraconal
Hemangiopericytoma
can have similar imaging appearance, but is rareSlide12
Optic Nerve Sheath Meningioma
Axial NECT image reveals a
calcified optic nerve sheath
menignioma
surrounding the
intraorbital
optic nerve resulting in
proptosis
.
Avid homogenous enhancement
is seen on axial MR T1W image. The
optic nerve
is normal in size but can have abnormal MR signal.
Enhancing mass encasing intraorbital
optic nerve with calcifications
Gradual onset of
proptosis
& decreased vision in middle-aged womenSlide13
Optic Nerve Glioma
Axial MR images of a patient with neurofibromatosis 1 show
T1
isointense
fusiform enlargement & kinking of the optic nerves. Note the
avid enhancement
of the right &
minimal enhancement
of the left optic nerve
gliomas
.
Fusiform optic nerve mass with variable involvement of posterior pathway
Variable enhancement
Bilateral
intraorbital
lesions are highly associated with NF1Slide14
CN III Schwannoma
Axial & coronal MR imaging shows a tubular,
intraconal
orbital mass with
low T1
/
high T2 signal
&
intense enhancement
in the superior orbital fissure extending posteriorly into the cavernous sinus. Note the
medial displacement of the tortuous CN II
.
Enhancing, tubular soft tissue mass along the course of
CN III with
smooth bony
remodeling
Can
have cystic formationSlide15
Lymphoma
MR imaging of the orbits in a patient with known anaplastic large cell lymphoma of the head, face & neck shows
increased T2 signal
with
enhancement
involving the
intraorbital
left optic nerve & surrounding
intraconal
fat. There is restricted diffusion of the optic nerve on
DWI
&
ADC map
.
Avidly enhancing soft tissue that molds to & encases orbital structures
Prompts whole body staging & surveillance for systemic lymphoma
Important differential consideration for any orbital massSlide16
Leptomeningeal Carcinomatosis
Axial post contrast T1W MR image reveals
symmetric enhancement of optic nerve sheaths &
intraconal
fat.
This was a histologically proven case of
leptomeningeal
carcinomatosis
in a 44
yo
female patient with HIV & metastatic
leiomyosarcoma
.Slide17
Orbital Carcinoid Tumor
Multiplanar
contrast-enhanced MR T1W images show
avidly enhancing
intraconal
mass
displacing the optic nerve medially
. This was a case of orbital metastasis from primary abdominal carcinoid tumor.
Represent 4%-5% of all orbital metastasis
May show elevated urinary 5-HIAA without hepatic metastasisSlide18
Extraconal Cavernous Hemangioma
MR imaging of the orbits illustrates a well-defined, right lateral
extraconal
mass with
high T2
,
low T1
signal intensity &
characteristic patchy enhancement.
Well-defined, ovoid, enhancing mass with patchy enhancement
Most common adult orbital mass, typically
intraconal
Hemangiopericytoma
can have similar imaging appearance, but is rareSlide19
CN V1 Schwannoma
Coronal & axial MR images demonstrate an orbital mass with
heterogeneous
high T2
signal
&
intense enhancement
in the right
superomedial
extraconal
space that displaces the globe &
superior rectus muscle
inferolaterally
. This was proven to be schwannoma in the expected course of CN V1.Slide20
Acute Myelogenous Leukemia
Axial & coronal MR imaging of the orbits in a pediatric patient with AML demonstrates
extraconal
soft tissue masses with
low T1
/
low
T2
signal intensity &
homogenous enhancement
.
Homogenous enhancing soft tissue in patients with known systemic disease
Extramedullary
hematopoeisis
can have similar appearance in same at-risk patient populationSlide21
Orbital Lymphoplasmacytic Lymphoma
Coronal & axial MR images of the orbits reveal a
homogenously,
enhancing
mass
with
low T1
/
high T2
signal intensity in the right superior
extraconal
compartment at the level of the lacrimal gland resulting in inferior displacement of the globe. Focus of
low T2W signal intensity
represents lymphoid tissue.Slide22
Wegener Granulomatosis
Axial & coronal MR imaging of the orbits demonstrates a medial
intraconal
soft tissue mass with
low T1
/
low T2
signal intensity &
avid enhancement
. This was a proven case of
orbital extension
of Wegener
granulomatosis
.
Systemic necrotizing
vasculitis
, with renal & respiratory involvement
Paranasal
sinus & orbital involvement (most common
extrasinonasal
site) with bone destruction, commonly bilateral
Difficult to differentiate from lymphoma or
sarcoidosis
on imagingSlide23
Orbital Subperiosteal Abscess
Axial CECT imaging through the orbits reveals a
subperiosteal
abscess
extending into the medial
extraconal
orbit & causing
displacement of the medial rectus
. Note the
ethmoid
sinusitis
.
P
eriorbital
edema & mild proptosis
are also evident.
Lenticular, rim-enhancing fluid collection along the medial
extraconal
orbit, with adjacent
ethmoid
sinusitis
Orbital cellulitis &
proptosis
; may be 1
st
sign of acute to
subacute sinusitis in childrenRestricted diffusion on MR increases diagnostic confidenceSlide24
Intraorbital Abscess
Axial CECT image of the orbits reveals right
proptosis
& lateral
periorbital
edema with
a rim enhancing fluid collection in the right lateral
extraconal
space
. Axial & coronal MR images demonstrate a
rim enhancing fluid collection
with
high T2W signal intensity
abutting & displacing the right lateral rectus muscle. There is restricted diffusion on
DWI
&
ADC
map
. Slide25
Lacrimal Lymphoma
Axial & coronal MR images reveal an enlarged,
intensely enhancing lacrimal gland mass
with
low T1
/
high T2
signal intensity. This was found to be diffuse large B-cell lymphoma of the lacrimal gland.
Pliable mass arising from lacrimal gland.
Can be multiple masses & predominantly MALT type Slide26
Lacrimal Gland Pleomorphic Adenoma
Multiplanar
MR images reveal an enlarged lacrimal gland with
low T1
/
low T2
signal intensity.
Unilateral, well-marginated, oval lacrimal mass with characteristic scalloped bony remodeling of lacrimal fossa
Slow growing & absence of painSlide27
Lacrimal Adenoid Cystic Carcinoma
Axial & coronal MR images reveal an
avidly enhancing
,
T2
hyperintense
heterogeneous mass with lobulated, well-defined margins arising from the lacrimal gland. Biopsy demonstrated adenoid cystic carcinoma of the lacrimal gland.
Irregular mass in the lacrimal fossa with bony erosion
Difficult to distinguish from benign lacrimal processes without bone destructionSlide28
IgG4 Related Disease
Bilateral chronic dacryoadenitis > submandibular sialadenitis >
parotiditis with variable orbital inflammatory pseudotumor
, myositis,
perineural
disease
Characteristically
hypointense
on T2WI due to high cellularity
&
fibrosis
Axial NECT image of the orbits reveal
enlarged lacrimal glands
. They demonstrate intermediate
T1
/
T2
signal intensity &
avid enhancement
.Slide29
Dacrocystocele
Axial NECT images of a 22-day-old newborn reveal a
cystic lesion
in the medial orbit at the location of the lacrimal sac. Note the
dilated nasolacrimal sac
.
Well-circumscribed cyst arising from the lacrimal sac, typically self-limited
25% bilateral with variable intranasal extension
Bilateral cysts may cause nasal obstruction at the level of inferior meatusSlide30
Dermoid Cyst
Axial imaging of the orbits reveals an ovoid, well-defined, right lateral
extraconal
mass causing medial displacement of the lateral rectus. This mass demonstrates
fatty attenuation (-20 HU)
,
hyperintensity
on T1W
, &
hypointensity
on contrast-enhanced T1W fat suppression
.
Well-circumscribed,
nonenhancing
unilocular
cystic lesion containing lipid
Can have capsular calcification Slide31
Extraconal Dermoid Cyst/Lipoma
Axial & coronal NECT images of the orbits reveal a
well-defined mass with fatty attenuation
along the lateral aspect of the left globe, anterior to the attachment of the lateral rectus muscle. Note the
punctate calcification
at the medial aspect of the mass, abutting the globe. Slide32
Extraocular Muscle Metastasis
Coronal & axial CECT images show an
enlarged, enhancing left lateral rectus muscle
with adjacent
conal
fat stranding. There is mild left
proptosis
. Axial & coronal MR images reveals
isotense
T1
/
hyperintense
T2
, &
avidly enhancing
lateral rectus muscle. The patient was a 31
yo
female with metastatic breast cancer & left orbital cellulitis not responding to antibiotics.Slide33
Idiopathic Inflammatory Pseudotumor
Axial & coronal MR imaging through the orbits shows a poorly-defined
T1
hypointense
/
T2
hyperintense
mass
with
heterogeneous enhancement
encasing the
medial rectus
with involvement of multiple compartments. There is mild
proptosis
& lateral displacement of the globe.
Ill-defined
masslike
enhancing soft tissue involving any compartment of the orbit; 25% bilateral
Diagnosis of exclusion; biopsy for atypical onset, poor response or recurrence
Typically painfulSlide34
Lymphangioma
MR imaging of the orbits shows an irregular, lobulated
retrobulbar
mass with characteristic
fluid-fluid levels
& multi-compartment involvement.
Low T1
/
heterogenous
high T2
signal intensity &
enhancement
are seen.
Ill-defined, lobulated lymphatic & venous malformation spanning multiple compartments
Characteristic fluid-fluid levels, blood products, & variable irregular enhancementSlide35
Metastatic Breast Cancer
Axial & coronal MR images show
T1
hypointense
,
enhancing metastatic breast cancer
filling multiple compartments of the bilateral orbits. Note the prominent
right
enophthalmos
secondary to classic
schirrous
changes. Slide36
SummaryIt is crucial for radiologists to be familiar with the imaging features of orbital masses. Some have characteristic findings, e.g. optic nerve
glioma, optic nerve sheath meningioma, cavernous hemangioma, etc. Compartmental approach to assessing orbital lesions helps guide diagnostic considerationCorrelation between imaging and physical findings are paramountSlide37
References
Ansari, Sameer A., and Mahmood F. Mafee. "Orbital cavernous hemangioma: role of imaging." Neuroimaging clinics of North America 15.1 (2005): 137-158. Chung, Ellen M., et al. "From the Archives of the AFIP Pediatric Orbit Tumors and Tumorlike
Lesions: Osseous Lesions of the Orbit 1." Radiographics 28.4 (2008): 1193-1214. Demirci, Hakan, et al
. "Orbital tumors in the older adult population
.“
Ophthalmology
109.2 (2002): 243-248
.
Kapur
,
Rashmi
, et al.
"Orbital schwannoma and neurofibroma: role of imaging." Neuroimaging Clinics of North America 15.1 (2005): 159-174.Smoker, Wendy RK, et al.
"Vascular Lesions of the Orbit: More than Meets the Eye 1." Radiographics 28.1 (2008): 185-204.Tailor, Tina D., et al. "Orbital neoplasms in adults: clinical, radiologic, and pathologic review." Radiographics 33.6 (2013): 1739-1758.
Uduma, Felix Uduma, and Kamga Titalom. "Intra-orbital malignant melanoma: role of MR imaging (a case report and literature review)." Global journal of health science 4.1 (2011): p253.Slide38
THANKS FOR VIEWING OUR PRESENTATION
Please send questions or comments to:
nguyenvd@uthscsa.edu