

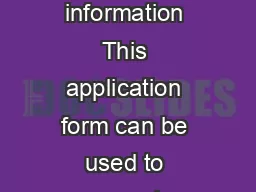
sign here INSTRUCTIONS Please fill out the entire form using BLACK ink Please write neatly using capital letters When complete answer the questionsat the bottom of the page and sign your name in ID: 828294
Download Pdf The PPT/PDF document "mm/dd/yyyyI verify that the above inform..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.





1 mm/dd/yyyyI verify that the above inform
mm/dd/yyyyI verify that the above information is correct. sign here INSTRUCTIONS: Please fill out the entire form using BLACK ink. Please write neatly using capital letters. When complete, answer the questionsat the bottom of the page and sign your name in the signature box.Are you or your dependents covered under another healthcare insurance program or policy OTHER THAN MILA'S CIGNA PLAN? YES Do you access the Internet from home? YES E-mail address (leave blank if none): First Name: Last Name: MI: Address 1: Address 2: City: State: Social Security Number: - - Sex: Employee Status: Active Retired Deceased EMPLOYEE RECORDMarital Status: Single Married Divorced WidowedDisabled: Yes Birth Date: / / Retirement Date: / / QUESTIONSAre you or your dependents entitled to benefits from Medicare? First Name: Last Name: MI: Dependent 1Social Security Number: - - Birth Date: / / First Name: Last Name: MI: Dependent 2Social Security Number: - - Birth Date: / / First Name: Last Name: MI: Dependent 3Social Security Number: - - Birth Date: / / First Name: Last Name: MI: Dependent 4Social Security Number: - - mm/dd/yyyyBirth Date: / / First Name: Last Name: MI: Dependent 5Social Security Number: - - Birth Date: / / Terminate Coverage?: Relation: Spouse Other Sex: Disabled: Student: Terminate Coverage?: Relation: Spouse Other Sex: Disabled: Student: Terminate Coverage?: Relation: Spouse Other Sex: Disabled: Student: Terminate Coverage?: Relation: Spouse Other Sex: Disabled: Student: Terminate Coverage?: Relation: Spouse Other Sex: Disabled: Student: mm/dd/yyyymm/dd/yyyymm/dd/yyyymm/dd/yyyy First Name: Last Name: MI: Dependent 6Social Security Number: - - mm/dd/yyyyBirth Date: / / First Name: Last Name: MI: Dependent 7Social Security Number: - - Birth Date: / / Terminate Coverage?: Relation: Spouse Other Sex: Disabled: Student: Terminate Coverage?: Relation: Spouse Other Sex: Disabled: Student: mm/dd/yyyyPlease return this form to:(If yes, please send us a photocopy of each Medicare card.) DATE MILA, 111 Broadway, 5th Floor, New York, NY 10006 5754473926