

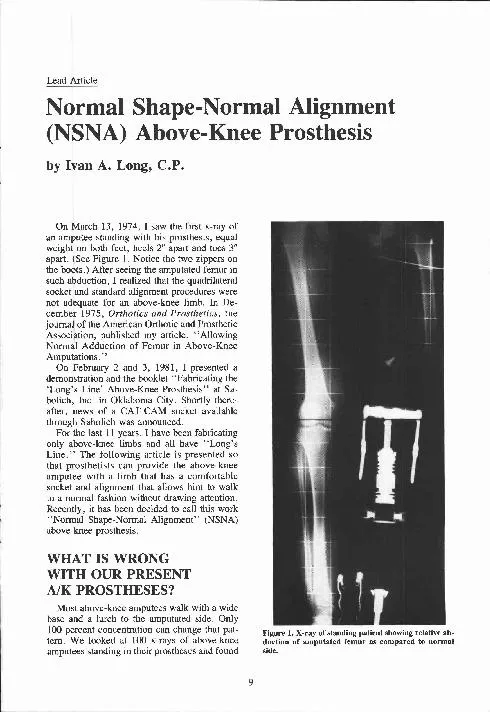
دم د نغم بهجة Maxillofacial Prosthetics the art and science of anatomic functional or cosmetic reconstruction by means of nonliving substitutes of those regions in the maxilla mandible and face that are missing or defective because of surgical interven ID: 910990
Download Presentation The PPT/PDF document "Maxillofacial Prosthetics" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


![Oral & Maxillofacial Pathology Journal [ OMPJ ]](https://thumbs.docslides.com/142170/oral-maxillofacial-pathology-journal-ompj.jpg)
Slide1
Maxillofacial Prosthetics
,
دم
د. نغم بهجة
Slide2Maxillofacial Prosthetics
Slide3“the art and science of
anatomic,
functional
,
or
cosmetic
reconstruction
by means of
nonliving substitutes of those regions in the maxilla, mandible, and face that are missing or defective because of surgical intervention, trauma, pathology, developmental or congenital malformations.”
Maxillofacial
prosthodontic
Slide4is an artificial device
used to replace missing
facial or oral structures.
Maxillofacial prosthesis
Slide5Reconstruct of missing parts in maxilla, mandible and face with prosthesis.
To achieve:
1- Preservation of residual structures.2- Reconstruction of function.
3-
Improvement in esthetic.
The Aim of Maxillofacial Prosthetic:
Slide6Artificial facial parts found on Egyptian mummies. Ancient Chinese known to have made facial restorations.
ancient-artificial-eye
Slide71
-Congental2
-Traumatic3-Pathological with radical surgery
1-
Intra Oral (Maxilla and Mandible).
2-
Extra Oral (eye, nose, ear).
Causes of Facial and oral Tissues loss
These factors result to 2 types of defects either:
Slide8-
Congenital
.Cleft lip..Cleft palate.-
Acquired
.Total maxillectomy
.Partial maxillectomy
Types of Maxillary Defects
Slide9Cleft lip occurs due to improper fusion between the fronto-nasal and maxillary process .
Cleft lip
&
palate
Slide10it is may be unilateral, bilateral and in Mohr's syndrome ,midline cleft lip is seen.
Slide11Cleft lip and the
combination of cleft
lip and cleft palate occur
twice
as often
in
males
as in females,
while cleft palate
alone occurs more
often in females.
Slide12Clefts occur most
often in children of
Asian, Latino or
Native American
These deformities
are known to occur
less frequently
in African, Americans
.
Slide13As a result of the abnormalities in the upper arch of the mouth,
teeth may
not erupt properly or may be missing completely. In such cases, artificial teeth and orthodontics (braces
) are usually required. Routine oral hygiene,
tooth
brushing
and
flossing
are still required to maintain healthy teeth and gums and prevent gum disease (periodontitis) and tooth decay.
Dental Problems
Slide14Treatments for Cleft Lip
and Cleft Palate
Slide15Children with cleft lip and/or cleft palate are treated over the course of
18 or more years
. Treatment can involve a team of professionals beginning shortly after birth and continuing throughout adolescence.
Slide16The treatment team includes
medical, dental and
other
healthcare specialists
who work together to address
the many different and
complicated needs specific
to the individual.
Slide17Most acquired defect occur due to
surgical resection of tumors
or trauma .Acquired Maxillary Defect
Slide18These are usually classified based on their extent
.
1.Total maxillectomy : both the maxillae are resected.
2
.Partial Maxillectomy
:
resection of one or a part of the maxilla or palate.
Types of Acquired
Maxillary defect
Slide19Obturator
•
Restores oro-nasal
partition
•
At times can be
added to prior
dentures
Slide20The
three types of prostheses are constructed for both edentulous and dentulous patients
Slide21Surgical Obturator
Interim Obturator Definitive Obturator
Slide22Slide23Slide24Materials Used in Maxillofacial
Reconstruction
Slide25POLY(METHYL METHACRYLATE)
Slide26it is the
most commonly used material for facial restoration but poor tear strength and life- less appearance have limited them from universal acceptance .
Silicones
Slide271-
HTV-Silicone : it requires
heat for vulcanization . It is highly viscous , white , opaque and has better physical properties .
Slide282-
RTV-Silicones : they are
room temperature polymerizing silicones . It is esear to process and allow intrinsic colouration .
Slide29Metal :
metal implants are used to obtain bone anchorage for
a prosthesis . Implant metals used are Titanium alloys , base metal alloys are used for denture base fabrication
Slide30Realistic coloration of extraoral prostheses is an
important feature
for patient
satisfaction
and
acceptability
.
Coloration
Slide31Intrinsic coloration involves incorporating precise proportions of pigments by mixing (RTV) or milling (HTV) into the base elastomer before to packing in the mold and curing in a dry heat oven.
Slide32In general, the extrinsic coloration uses a medical-grade adhesive combined with xylene and earth pigments, which are applied to the external surface of the prosthesis. The prosthesis is then postcured in a dry heat oven to evaporate the xylene.
Extrinsic coloration
Slide33Slide34Fabrication Of
the Prostheses
Slide35The method for fabricating a prosthesis is similar for most materials.
An impression is made of the affected area with alginate. A master cast is
poured, duplicating the defect on the patient.
Slide36Step 1
- Seat patient comfortably, cover hair and coat eyebrows with cold cream to prevent entrapment of alignate.
Slide37Step 2
- Alignate mixed. Patient learns hand signals protocol to communicate. Pouring of alignate on forehead to allow for flow down the face.
Slide38Step 3
- Alignate poured taking care not to entrap air in anatomical undercut areas. Incase the patient is traumatized (children or burns victims with painful skins) by process anaesthesia is needed.
Slide39Step 4
- Guaze stockinet is removed from patients hair.Impression is removed from patients face (allowing time for patients eyes to adjust to light in the room
Slide40Step 5
- Impression disinfected. Air passage blocked in impression. Exposed plaster coated with petroleum jelly to prevent bonding with stone cast. Stone allowed to gently flow over the surface of the alignate.
Slide41Step 6
- Stone cast may need trimming on model trimmer.
Slide42Slide43Slide44Slide45Slide46Fabrication of a Maxillofacial Prosthesis Using a Computer-Aided Design and Manufacturing System
Slide47Seat patient comfortably, Adjust receiver on patients head. Scanner imaging, Polhemus FastScan digital scanner
Slide48Slide49Maxillofacial prostheses are usually fabricated on the basis of impressions made with dental-impression material.
The extent to which the prosthesis reproduces normal facial morphology depends on the clinical judgment of the individual fabricating the prosthesis.
Slide50This new technique describes a
computer-aided design and manufacturing system
(CAD/CAM) for the fabrication of maxillofacial prostheses. This system will provide a more consistently accurate reproduction of facial morphology
.
Slide51Facial measurements were taken using a non-contact three-dimensional laser morphological
measurement system.
Slide52The measurements were sent to a computer numerical controlled
(
CNC) milling machine to generate
a cast of the patient's face for the
fabrication of prosthesis
.
Slide53Facial contours were measured using a laser. This method minimizes
patient discomfort and avoids soft tissue
distortion by impression material. Moreover, the digital data obtained is easy to store and transmit, and
mirror-images can be readily generated by computer processing
.
Results
Slide54This method offers an objective, quantified approach for fabricating maxillofacial prostheses
.
Conclusion
Slide55Retention of
maxillofacial prostheses
Slide56Retention of facial prostheses has been primarily by way of
medical adhesives. An ideal adhesive should be one that provides firm functional retention under flexure or extension during speech, facial expressions, and moisture or perspiration contact.
Slide57Adhesives for extraoral maxillofacial prostheses require a substantial amount of supportive ingredients properly formulated to provide lasting viscoelasticity with a high degree of retention. Numerous brand names of adhesives have been introduced over the years in maxillofacial prosthetics.
Slide58Other methods of retention include engagement of anatomic tissue undercuts, thereby minimizing dependence on adhesives.
The potential for tissue irritation exists with this technique, and therefore it must be used prudently.
Areas that have been irradiated contraindicate the use of this technique.
Slide59Finally
, with the increaed use of
osseointegrated implants, dependence on adhesive and anatomic methods of retention has diminished.
Slide60Magnets
can be used to minimize force transfer to the implant and supporting bone. The resultant decrease in dependence on chemical (adhesives) and anatomic (tissue undercuts) sources of retention is beneficial to both the patient and the prosthetic rehabilitation.
Slide61Anterior view of the
anatomical defect
following maxillectomy
Oblique view of the anatomical
defect showing communication
with nasal cavity
.
Slide62Location of magnet placement between
the facial prosthesis extension and the
palatal obturator denture.
Slide63Positioning of the retention
magnets
Highligher paste on thesuperior aspect of the
palatal obturator prosthesis
.
B
.
Transfer of the paste to
the facial prosthesis
extension to demarcate the
location for the secondmagnet.
Slide64Facial prosthesis in place after
one year of use.
Slide65SURVEILLANCE
One of the biggest advantages in using removable prostheses in the head and neck cancer patient is the ability to provide tumor surveillance. As the overall survival of head and neck cancer approaches 52%, there is a window of time to monitor for local recurrent lesions. With use of prostheses, it becomes possible to directly visualize recurrent areas that may be apparent in the perioperative period to the third year of
follow-up. If these areas are reconstructed with tissue, the ability to provide surveillance is markedly reduced.
Slide66Grateful
for
Patient Lestining