
08251992COVA HealthAware Flu Shot outside of the program for HRAgdhjgfgdsfggfhgsfhghdggfvgdgfghgdfghsdgfhgdgfdgfjg082519920825199208251992DOCUMENTATION ORT FLU VACCITIRECEIVED OUTSIDE THE ST ID: 862355
Download Pdf The PPT/PDF document "gjkfjghfdhgfhdjghfjkhvbfghdjhdjgvhjdhgjf..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




1 gjkfjghfdhgfhdjghfjkhvbfghdjhdjgvhjdhgjf
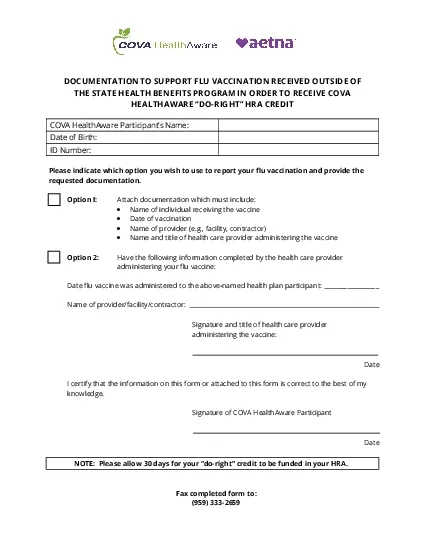
gjkfjghfdhgfhdjghfjkhvbfghdjhdjgvhjdhgjfhCOVA HealthAware - Flu Shot outside of the program for HRACOVA HealthAware - Flu Shot outside of the program for HRAgjhfdghfjhg 08/25/1992 COVA HealthAware - Flu Shot outside of the program for HRAgdhjgfgdsfggfhgsfhghdggfvgdgfghgdfghsdgfhgdgfdgfjg 08/25/1992 08/25/1992 08/25/1992 DOCUMENTATION ORT FLU VACCITIRECEIVED OUTSIDE THE STA BENEFI PROGRAM IN ORDER TO COVA HealAware Pticipa’s Nam Date of Birth: ID Number: Please indicate whi option you wi to use to report youflu ation and prove the reested docuntation. ion Attach do of individu receing the neDate of vaination of provider (e.g., facility, contrar) ion 2:ve the following information compled by e heth care proer adring your flu vaine: of provider/facility/contracr: Signature and title of th care proder Da certify the infotion n this form or aached to this fo is correct to e best of my nowlge. Signature of Da Please als foto be fued in your HRA. Fax completed fo: (959) 3332659 ____________ DOCUMENTATION ORT FLU VACCITIRECEIVED OUTSIDE THE STA BENEFI PROGRAM IN ORDER TO RECEIVE COVA HEALAWARE “DO-RIGHT” HRA DIT COVA HealAware Pticipa’s Nam Date of Birth: ID Number: Please indicate whi option you wi to use to report youflu ation and prove the reested docuntation. ion Attach docuntation which must includ of individu receing the neDate of vaination of provider (e.g., facility, contrar) and title of health care provider administing the ion 2:ve the following information compled by e heth care proer adring your flu vaine: Date flu ine w adred to the above-nd th plan participant of provider/facility/contracr: Signature and title of th care proder adring the ine: Da certify the infotion n this form or aached to this fo is correct to e best of my nowlge. Signature of COVA HethAware Participant Da Please als foto be fuin your HRA. Fax completed fo: (959) 3332659 ____________ 08/25/1992 08/25/1992 08/25/1992 654sd65sa4d5as4dsa5d4saCOVA HealthAware - Flu Shot outside of the program for HRAgdhjgfgdsfggfhgsfhghdggfvgdgfghgdfghsdgfhgdgfdgfjg 08/25/1992 DOCUMENTATION ORT FLU VACCITIRECEIVED OUTSIDE THE STA BENEFI PROGRAM IN ORDER TO RECEIVE COVA HEALAWARE “DO-RIGHT” HRA DIT COVA HealAware Pticipa’s Nam Date of Birth: ID Number: Please indicate whi option you wi to use to report youflu ation and prove the reested docuntation. ion Attach docuntation which must includ of individu receing the neDate of vaination of provider (e.g., facility, contrar) and title of health care provider administing the ion 2:ve the following information compled by e heth care proer adring your flu vaine: Date flu ine w adred to the above-nd th plan participant of provider/facility/contracr: Signature and title of th care proder adring the ine: Da certify the infotion n this form or aached to this fo is correct to e best of my nowlge. Signature of COVA HethAware Participant Da Please als foto be fued in your HRA. Fax completed fo: (959) 3332659 ____________ DOCUMENTATION ORT FLU VACCITIRECEIVED OUTSIDE THE STA BENEFI PROGRAM IN ORDER TO RECEIVE COVA HEALAWARE “DO-RIGHT” HRA DIT COVA HealAware Pticipa’s Nam Date of Birth: ID Number: Please indicate whi option you wi to use to report youflu ation and prove the reested docuntation. ion Attach docuntation which must includ of individu receing the neDate of vaination of provider (e.g., facility, contrar) and title of health care provider administing the ion 2:ve the following information compled by e heth care proer adring your flu vaine: Date flu ine w adred to the above-nd th plan participant of provider/facility/contracr: Signature and title of th care proder adring the ine: Da certify the infotion n this form or aached to this fo is correct to e best of my nowlge. Signature of COVA HethAware Participant Da Please als foto be fued in your Fax completed fo: (959) 3332659 ____________