
Carl Kraus MD Rama S Ayyala MD Jonathan K Kazam MD Tony T Wong MD Presented as an educational exhibit at the 2016 RSNA Annual Meeting MK235EDX Address correspondence to Tony T Wong MD ID: 815401
Download The PPT/PDF document "Imaging of Juvenile Hip Conditions Predi..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
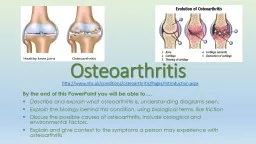
Imaging of Juvenile Hip Conditions Predisposing to Premature Osteoarthritis
Carl Kraus, MD, Rama S. Ayyala, MD, Jonathan K. Kazam, MD, Tony T. Wong, MD
Presented as an educational exhibit at the 2016 RSNA Annual Meeting, MK235-ED-X
Address correspondence to:Tony T. Wong, MDDepartment of Radiology New York Presbyterian Hospital/Columbia University Medical Center630 W 168th St, MC-28, New York, NY 10032ttw2105@cumc.columbia.edu
All authors have disclosed no relevant relationships
.
An earlier incorrect version of this presentation appeared online. This presentation was
corrected on December 21, 2017.
Slide2Background
Osteoarthritis of the hip is a major cause of morbidity and mortality in the United States affecting more than 54 million adults.
Causes of Hip OsteoarthritisJuvenile Prearthritic ConditionsDevelopmental dysplasia of the hip (DDH)Legg-Calvé-Perthes disease (LCP)Slipped capital femoral epiphysis (SCFE)Proximal femoral focal deficiency (PFFD)Femoroacetabular impingement (FAI)Other CausesCoxa valga and varaInfection
Trauma (eg, hip dislocation, pelvic fractures)Systemic disease (eg, rheumatoid arthritis)Imaging is important for diagnosis of the prearthritic
conditions and to evaluate their long-term complications.
Total costs associated with arthritis and related conditions are approximately $128 billion per year.
Slide3Learning Objectives
Review hip embryology and developmentDiscuss epidemiology, clinical information, imaging, and treatment of juvenile
prearthritic hip conditions (DDH, LCP, SCFE, PFFD, FAI)Identify long-term complications of these conditions
Slide4Hip Embryology and Development
Fetal
4 weeks: Limb buds form8 weeks: Cartilaginous model for the acetabulum and femur form11 weeks: Infantile configuration of the acetabulum and femoral head form16 weeks: Femoral ossification is complete to the level of the greater trochanterInfancyFemur forms by appositional growth from defined growth zones Longitudinal growth plate (red arrow) Trochanteric growth plate (yellow arrow) Femoral neck isthmus (green arrow)
ChildhoodAcetabulum grows appositionally through the articular cartilage (arrowheads) and interstitially through the triradiate cartilage (
star
).
Reciprocal interactions between the acetabulum and the femoral head are essential for proper structure and function in adulthood.
Ossified bone
Growth cartilage
Slide5Developmental Dysplasia of the Hip
Background
A spectrum of abnormalities present at birth or during infancy, which range from mild acetabular dysplasia to hip subluxation or dislocation.EpidemiologyIncidence: 1–66 per 1000 live births
Risk factors for development - Female sex (6:1 female-to-male ratio) - Breech presentation - Family history of DDHBilateral in 33% of patientsClinical Information
Abnormal neonatal examination
Barlow maneuver
- Clunk with posterior-directed pressure with hips adducted and flexed
Ortolani maneuver
- Clunk with hip abduction in flexed position
Galeazzi test
- Limb length discrepancy with differential knee height
Slide6Developmental Dysplasia of the Hip
Imaging Appearance—Ultrasonography (US)
Imaging modality of choice for DDH evaluation (sensitivity, 88.5%; specificity, 96.7%)Performed after 4–6 weeks of age (may be falsely positive earlier because of ligamentous laxity from maternal hormones)
Coronal view
Transverse view (hip flexed to 90
°
)
Ischium
Labrum
Femoral
head
Ilium
Acetabular
roof
Triradiate
cartilage
Femoral
head
Femoral
shaft
Labrum
Slide7Developmental Dysplasia of the Hip
Imaging Appearance—US
αAlpha angle = 75°
Alpha angle = 35°
How to measure alpha angle
Obtain coronal US image
Identify center of femoral head (white circle)
Draw line parallel to the ilium (
red
)
Draw line through the roof of the acetabulum (
green
)
Normal alpha angle greater than 60°
Normal Hip
Dysplastic Hip
Slide8Developmental Dysplasia of the Hip
Imaging Appearance—Radiographs
Normal location of the femoral head (dotted circle) is within the inferomedial quadrant formed by the intersection of Hilgenreiner and Perkin lines.
Hilgenreiner
line
:
Drawn horizontally through the superior aspect of both
triradiate
cartilage
Perkin line
:
Drawn perpendicular to
Hilgenreiner
line, intersecting the lateral most aspect of the acetabular roof
Acetabular line:
Drawn connecting the superolateral acetabular roof to the ipsilateral
triradiate
cartilage (angle formed with horizontal line should be less than 30°)
Shenton arc:
Curvilinear line drawn connecting the obturator foramen and the medial aspect of the proximal femoral metaphysis (line should be smooth and uninterrupted)
Neutral frontal radiographs are obtained after 6 months of age (when femoral heads are ossified).
Dysplastic
Normal
Slide9Developmental Dysplasia of the Hip
Treatment
Majority of cases treated nonoperativelyWith early diagnosis, treatment success rate is approximately 95%.Pavlik harness—maintains abduction and external rotationSurgical treatment reserved for refractory disease or late diagnosesOpen reduction and spica castPeriactebular osteotomycorrect shallow acetabulum
Derotational femoral varus osteotomy—improve femoral head coverage
Periacetabular osteotomy
Derotational
osteotomy: Removed bone (green triangle) resulting in improved femoral head coverage (red arcs).
Slide10Developmental Dysplasia of the Hip
Long-term ComplicationsMagnetic resonance (MR) arthrograms obtained 12 years later in a 15-year-old adolescent girl (same patient) with hip pain. Note dysmorphic femoral head shape and undercoverage (star), torn hypertrophied labrum (arrow), and paralabral cyst (arrowhead).
Anteroposterior radiograph in a 3-year-old girl with mild hip dysplasia shows small femoral head (star) and shallow acetabulum (arrow).
Early-onset arthritis
Labral hypertrophy and tear
FAI
Coronal T1-weighted fat-saturated
Coronal proton-density–weighted
Slide11Developmental Dysplasia of the Hip
Long-term Complications
17 months old 4 years old
6 years old 12 years oldSerial radiographs in a female child with treated DDH demonstrate progressive deformity and early-onset arthritis despite multiple femoral and pelvic osteotomies.
Slide12Legg-Calvé-Perthes
Disease BackgroundIdiopathic avascular necrosis of the femoral head epiphysis
EpidemiologyMale-to-female ratio: 4:1Peak incidence between 4 and 8 years old10% successive bilateral involvement-Usually at different stagesClinical InformationCommonly manifests as painful limpTrauma may be inciting factor that unmasks or accentuates chronic pain.60%–70% heal without functional impairment at maturityBetter prognosis for presentation at age younger than 6 years and less resultant femoral head flattening
Slide13Legg-Calvé-Perthes
Disease Imaging Appearance—RadiographsWaldenstr
öm stages of PerthesStage 1 InitialStage 2 FragmentationStage 4 HealedStage 3 Reossification
Periarticular osteoporosis → Small and dense femoral ossification center → Early lateral displacement of epiphysis and medial joint widening → Subchondral fracture crescent sign (arrow)
More lateral extrusion (double-headed arrow) with epiphyseal flattening, fragmentation, sclerosis, and areas of resorption (arrowheads)
New bone formation (curved arrow)
Reconstitution of femoral head with or without residual deformity
Slide14Legg-Calvé-Perthes
Disease Imaging Appearance—RadiographsStulberg
classification: Assess for risk of developing osteoarthritis in the future1. Normally contoured femoral head2. Spherical femoral head with coxa magna, short femoral neck, and/or steep acetabulum3. Ovoid femoral head with coxa magna, short femoral neck, and/or steep acetabulum4. Flattened femoral head with abnormal femoral neck and abnormal acetabulum5. Flattened femoral head with normal neck and normal acetabulum
Stage 1
Stage 2
Stage 3
Stage 4
Stage 5
Normal Mild arthritis Moderate arthritis Severe arthritis
Slide15Legg-Calvé-Perthes
DiseaseAvascular PhaseNecrotic portions of femoral head - Low T1 signal intensity
- Variable T2 signal intensity (high initially from edema then low with advanced necrosis)Partial or complete nonenhancement of epiphysisSubchondral collapseJoint effusion with synovitisRevascularization and Reparative PhaseVariable epiphyseal signal abnormality reflecting different areas of residual necrosis and revascularizationMay see epiphyseal hyperenhancementMetaphyseal cysts and edemaPhyseal undulationJoint effusion with synovitis Imaging Appearance—MR Imaging
MR images in a 2-year-old boy in the avascular phase. Note marked flattening of femoral head epiphysis and nonenhancement (arrows).Coronal postcontrast T1-weighted fat-saturated
Coronal T1-weighted
MR images in a 7-year-old boy in the revascularization phase show mixed epiphyseal signal intensity (arrowheads), metaphyseal cyst and edema (arrow), and effusion (curved arrow).
Coronal T2-weighted fat-saturated
Coronal T1-weighted
Slide16Legg-Calvé-Perthes
Disease Treatment
Treatment is dependent on age, degree of femoral head involvement, and stage of disease.Age younger than 6 years: Nonsurgical with motion restriction and altered weight bearingAge older than 8 years Early stage: Femoral or pelvic osteotomies to improve femoral head containment Late stage: Osteotomies and possible external fixation with distraction to offload hipOlder adolescents: May be treated similar to adult avascular necrosis with core decompression and vascularized bone graft or total hip arthroplastyFemoral varus osteotomyAcetabular innominate osteotomy
Core decompression and vascularized fibular graft
Distraction with external fixator
Slide17Legg-Calvé-Perthes
Disease Long-term Complications
Early-onset arthritis—most common complicationLabral tearsOsteochondral lesions and intra-articular bodiesFAIPhyseal barsStulberg Stage 4MR arthrograms obtained 4 years after radiograph in an 18-year-old man with chronic hip pain. Note acetabular cartilage delamination (arrowheads), osteochondral fragmentation (bracket), subchondral cysts and edema (curved arrow), and anterosuperior labral tear (straight arrow).
Sagittal T1-weighted fat-suppressedCoronal proton-density–weighted
Slide18Legg-Calvé-Perthes
Disease Long-term Complications
Frontal radiographs at 5-year follow-up in a boy who underwent acetabular and femoral osteotomies. Note ovoid femoral head with loss of sphericity. MR arthrograms obtained at 14 years old. Note osteochondral lesion in the femoral head with disruption of subchondral bone plate and tiny subchondral cysts (arrows).
9 years old14 years old Sagittal T1-weighted fat-saturated
Sagittal T1-weighted fat-saturated
Slide19Slipped Capital Femoral Epiphysis
Background
Fracture through the proximal femoral physis due to mechanical shear forcesEpidemiologyMost common hip disorder in adolescence
Peak ages: 12 years in girls and 14 years in boysMale-to-female ratio: 2.5:1African-American–to-white ratio: 4:1Bilateral in 10%Other side often involved within 2 years of first side
Clinical Information
Adolescent with limp and hip pain
Often no trauma history
Obesity is strong risk factor
May have predisposing metabolic abnormality such as hypo- or hyperparathyroidism and renal failure
Unstable hips have high risk of avascular necrosis
Clinical Grading of Stability
Stable: ability to bear weight
Unstable: inability to bear weight
Slide20Slipped Capital Femoral Epiphysis
Imaging Appearance—Radiographs
Normal Hip
Abnormal signs on anteroposterior viewDecreased epiphyseal height (
yellow double-headed arrow
)
Klein line: Line along the lateral femoral neck does not intersect epiphysis (
red line
)
Capener
triangle: Loss of normal overlap at medial femoral metaphysis and ischium (triangle)
Abnormal Hip
Slide21Slipped Capital Femoral Epiphysis
Imaging Appearance—Radiographs
Southwick MethodOn frog-leg lateral viewA. Line connecting anterior and posterior physeal marginsB. Line perpendicular to AC. Line parallel to femoral neckLateral epiphyseal-shaft angle (LESA) (red) is angle between B and C. Southwick angle is difference of LESA between affected and unaffected side (>30° difference is abnormal)
A
B
C
Staging of SCFE according to Southwick angle
Grade 1 (mild): 0°–30
°
Grade 2 (moderate): 30°–50
°
Grade 3 (severe): >50
°
Frog-leg lateral
Slide22Slipped Capital Femoral Epiphysis
Imaging Appearance—MR Imaging
Can be helpful to identify preslip or radiographically occult SCFEFindings include edema and/or widening of the physis with surrounding epiphyseal and metaphyseal marrow edemaMR images in a 12-year-old girl with hip pain show displacement of epiphysis posterior to femoral neck (curved arrow), no intersection at Klein line (dotted line), and physeal edema (arrowheads).
Axial T2-weighted fat-saturated
Coronal T1-weighted
Coronal T2-weighted fat-saturated
Slide23Slipped Capital Femoral Epiphysis
TreatmentOptions
Pinning—can be done with all stable and unstable slips (usually in situ)Epiphyseal reduction—controversial and reserved for unstable early slips (<24 hours)Proximal femoral osteotomy—correction of chronic deformity from a severe slipContralateral prophylactic pinningcontroversial and considered for high-risk patients (age < 10 years, endocrinopathy, contralateral pain) Serial radiographs in a 9-year-old girl with acute unstable slip.
A, Epiphyseal displacement with physeal widening. B, Reduction and pinning. C, Restricted range of motion requiring valgus osteotomy.Initial presentation
Less than 24 hours later
8 years later
A
C
B
Slide24Slipped Capital Femoral Epiphysis
Long-term ComplicationsEarly-onset arthritisAvascular necrosis
Labral tears4. FAI5. Limb length discrepancyMR arthrograms in an 18-year-old woman with prior SCFE and hip pain show femoral cam deformity with large alpha angle, early-onset arthritis with apposing cartilage wear (arrowheads), and anterosuperior labral tear (arrow).
α
= 85°
Axial oblique proton density weighted
Coronal T1-weighted fat-saturated
Sagittal T1-weighted fat-saturated
Slide25Proximal Focal Femoral Deficiency
Background
Congenital deformity characterized by a shortened femur and varying degrees of femoral head and acetabular deficiencyEpidemiologyIncidence: One in 52,000 live births
Third most common longitudinal lower extremity deficiency Bilateral in 10%–15% Clinical InformationCan often be diagnosed on prenatal US image
Shortening of affected limb(s)
Associated abnormalities: Fibular hemimelia (80%),
tibial
shortening, coxa
vara
, lower extremity contractures, knee ligamentous laxity and/or deficiency, and foot deformities
Slide26Proximal Focal Femoral Deficiency
Imaging Appearance—RadiographsAitken Classification
ClassFemoral HeadAcetabulumFemoral ShaftAPresentNormalShortened with varus subtrochanteric deformityBPresent, but delayed ossificationMild to moderately dysplasticShortened with proximal bony tuft; no subtrochanteric connection between head and shaft
CAbsent Severe dysplasiaComplete absence of trochanteric area and shorter shaft than B with bony tuftD
Absent
Absent (flat)
Severely short with pointed proximal end and no tuft
Class A
Class B
Class C
Class D
Slide27Proximal Focal Femoral Deficiency
Imaging Appearance—Radiographs
Frontal pelvic radiograph in a 2-year-old girl with Aitken class A PFFD on the right. Note varus shaft deformity (arrow), shortened femur (bracket), and asymmetrically smaller femoral head (dotted circles).Side-by-side frontal hip radiographs in a 31-year-old woman with bilateral Aitken class C PFFD. Note absence of femoral heads, proximal bony tufts (arrows), shortened femora (brackets), and severely dysplastic acetabuli (dotted lines).
Slide28Proximal Focal Femoral Deficiency
Imaging Appearance—MR ImagingCan identify presence of femoral head prior to time of ossification to differentiate between Aitken class A and B versus C and D
Also useful for evaluation of acetabular dysplasia, joint congruency, labral hypertrophy, proximal femoral physis, hip impingement, and fibrocartilaginous connection between head and shaft
MR images in a 6-month-old male infant with left PFFD and no femoral head on radiograph. Unossified femoral head is located in the acetabulum (bracket). Tiny ossification center (arrow) is present, though asymmetrically smaller than right side (arrowhead).
Coronal gradient-echo
Sagittal gradient-echo
Slide29Proximal Focal Femoral Deficiency
Treatment
Individualized goals based on severity of deformity, expected limb length discrepancy (ELLD), and associated abnormalitiesNonsurgical management: mild or bilateral deformitiesSurgical management: staged surgeries to equal limb lengths (less severe deformities with ELLD < 20 cm) or fit for prosthesis (ELLD > 20 cm) 7 months old: Aitken class A PFFD on left side2 years old: Femoral valgus osteotomy, Dega osteotomy in acetabulum
6 years old: Second lengthening osteotomy4 years old: Lengthening osteotomyFemale child at four ages
Slide30Proximal Focal Femoral Deficiency
Long-term ComplicationsLimb length discrepancy
Hip impingementEarly onset arthritisStanding frontal radiograph in a 10-year-old girl who underwent distal femoral epiphysiodesis on normal right side for limb length discrepancy after multiple left-sided osteotomies.Frog-leg lateral radiographs at 11-year follow-up in female patient with PFFD, fibular hemimelia, and absent foot show greater trochanteric-iliac impingement (arrow) after multiple staged osteotomies and prosthesis placement.1 day old
11 years old
Slide31Femoroacetabular Impingement
BackgroundEpidemiologyMale-to-female ratio: 14:1 (cam), 1:3 (pincer)
In adolescents, the age range is 13–18 years old.Clinical InformationPain commonly in groin, anterior thigh, and lateral hipCatching or popping may be described when there is associated labral injury.Fifty–fifty insidious versus acute onsetUsually associated with high-demand sports, such as aerobics, dancing, football, and soccerAltered osseous morphology that causes pain because of abnormal contact between the femur and acetabulum during motion
Slide32Femoroacetabular Impingement
Background
1. Cam typeOsseous prominence at femoral head–neck junction 2. Pincer typeOsseous prominence at acetabulum3. Mixed typeOsseous prominence at both femoral head–neck junction and acetabulum
Normal
Cam
Pincer
Mixed
Slide33Femoroacetabular Impingement
Cam Deformity in the Adolescent PatientA severe deformity seen as a long-term consequence of one of the previously discussed pediatric hip abnormalities (hip dysplasia, SCFE, and LCP) OR
2. A mild deformity related to an abnormal developmental process that has been linked to vigorous sporting activity Background
Slide34Femoroacetabular Impingement
Multiple views (anteroposterior, frog-leg lateral, Dunn, and false profile) in a standard impingement series each profile the femoral head–neck junction at a different angle.Cam lesion may be identified on any view but is usually best seen on the frog-leg lateral or Dunn views (yellow dotted line
). Imaging Appearance—Radiographs for Cam AssessmentFrog-leg lateral45° Dunn
Slide35Femoroacetabular Impingement
Imaging Appearance—Radiographic Adequacy to Assess for Acetabular Pincer
Must be anteroposterior view of pelvis
Coccyx centered with tip 1–3 cm from superior margin of symphysis (double-headed arrow)
Symmetric obturator foramina (black circles)
Symmetric iliac wings (yellow lines)
Slide36Femoroacetabular Impingement
On anteroposterior view of pelvisNormal: Anterior acetabular wall (red dotted line) is medial to posterior wall (yellow line).
Pincer (focal overcoverage): Cranial acetabular retroversion: Anterior acetabular wall is lateral to posterior wall. Imaging Appearance—Radiographs for Pincer Assessment
Anteroposterior
Anteroposterior
Normal
Pincer
Slide37Femoroacetabular Impingement
On anteroposterior view of pelvisNormal: Acetabular wall (dotted red line) and femoral head (yellow line
) are lateral to ilioischial line (black line).Pincer (global overcoverage): Coxa profunda: Acetabular wall is medial to ilioischial line. Acetabular protrusio: Acetabular wall and femoral head are medial to ilioischial line. Imaging Appearance—Radiographs for Pincer Assessment
Anteroposterior
Anteroposterior
Anteroposterior
Slide38Femoroacetabular Impingement
Labral TearsAbnormal morphology or increase in signal intensity, contrast material imbibition
Typically in anterosuperior quadrantCartilage AbnormalitiesFocal defects, fissuring, or delaminationTypically adjacent to labral tear Imaging Appearance—MR ImagingMR arthrograms show labral tear with contrast material imbibition (arrows) and paralabral cyst (arrowhead).
Sagittal T1-weighted fat-saturated
Coronal proton-density–weighted
Sagittal T1-weighted
fat-saturated
Coronal T1-weighted fat-
saturated
MR arthrograms show labral tear with contrast material imbibition (arrow) and full-thickness cartilage defect (bracket).
Slide39Femoroacetabular Impingement
Osseous AbnormalitiesQuantify cam lesion with alpha angle on axial oblique image.
Abnormal alpha angle is greater than 55°. Cysts may be seen at femoral head–neck junction. Imaging Appearance—MR ImagingAlpha angleDraw best-fit circle around the femoral head.Draw line from center of circle bisecting femoral neck.Draw line from center of circle to the portion of neck that exits the circle.
α
Axial oblique proton-density–weighted
Axial oblique proton-density–weighted
Axial oblique proton-density–
weighted
MR arthrogram shows severe cam deformity from prior SCFE (arrow) and old tracks from prior pinning (arrowheads).
MR arthrogram shows mild cam deformity with small focus of underlying fibrocystic change (arrow).
Slide40Femoroacetabular Impingement
Treatment
Hip arthroscopyFemoroplasty—cam resectionAcetabuloplasty—pincer resectionLabral repair
α
Axial oblique proton-
density–weighted
α
Axial oblique proton-density– weighted
Frog-leg lateral radiographs (top) and MR arthrograms (bottom) in an 18-year-old man after hip arthroscopy show cam resection with interval decrease in alpha angle and restoration of normal femoral head–neck contour (red line).
Slide41Femoroacetabular Impingement
Long-term Complications
Sagittal T1-weighted fat saturated Coronal proton-density weightedTheorized to be cause of early-onset osteoarthritis in young adultsFrontal radiographs in a 32-year-old man with chronic pain show cam deformity with moderate joint space narrowing requiring total hip arthroplasty 8 months after initial presentation.
MR arthrograms in a 32-year-old man with chronic pain show labral tear (arrows) with arthritis and moderate apposing cartilage wear (arrowheads).
Slide42Summary
DDH is a spectrum ranging from mild acetabular dysplasia to hip subluxation or dislocation.LCP is idiopathic avascular necrosis of the femoral head epiphysis.
SCFE is a fracture through the proximal femoral physis.FAI is an alteration in osseous morphology that causes abnormal contact in the hip.PFFD is characterized by a shortened femur and varying degrees of femoral head and acetabular deficiency.All of these entities can result in early-onset arthritis because of altered anatomy.Imaging is important for initial diagnosis and to evaluate long-term complications.
Slide43Suggested Readings
Atweh LA, Kan
JH. Multimodality imaging of developmental dysplasia of the hip. Pediatr Radiol 2013;43(suppl 1):S166–S171. Bedoya MA, Chauvin NA, Jaramillo D, Davidson R, Horn D, Ho-Fung V. Common patterns of congenital lower extremity shortening: Diagnosis, classification, and follow-up. RadioGraphics 2015; 35(4):1191–1207.Biko DM, Davidson R, Pena A, Jaramillo D. Proximal focal femoral deficiency: evaluation by MR imaging. Pediatr Radiol 2012;42(1):50–56.Bracken J, Ditchfield M. Ultrasonography in developmental dysplasia of the hip: what have we learned? Pediatr Radiol 2012; 42(12):1418–1431. Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-Hayes M, Prather H. Clinical presentation of patients with symptomatic anterior hip impingement. Clin Orthop Relat Res 2009;467(3):638–644.Cooper AP, Doddabasappa SN, Mulpuri K. Evidence-based management of developmental dysplasia of the hip. Orthop Clin North Am 2014;45(3):341–354. Dillman JR, Hernandez RJ. MRI of Legg-Calve-Perthes disease. AJR Am J Roentgenol 2009;193(5):1394–1407. Jarrett DY, Matheney T, Kleinman PK. Imaging SCFE: diagnosis, treatment and complications.
Pediatr Radiol 2013;43(suppl 1):S71–S82.Phillppon MJ, Maxwell RB, Johnston TL, Schenker M, Briggs KK. Clinical presentation of femoroacetabular impingement. Knee Surg Sports Traumatol Arthrosc 2007;15(8):1041–1047.Sink EL, Gralla J, Ryba
A, Dayton M. Clinical presentation of
femoroacetabular
impingement in adolescents. J
Pediatr
Orthop
2008;28(8):806–811.
Tannast M, Siebenrock
KA, Anderson SE.
Femoroacetabular
impingement: radiographic diagnosis-what the radiologist should know. AJR Am J
Roentgenol
2007;188(6):1540–1552.
Uglow
MG, Clarke NM. The management of slipped capital femoral epiphysis. J Bone Joint
Surg
Br 2004;86(5):631–635.