
By DrSalauddin Pulmonary thromboembolism One clot or many clots that migrate from systemic circulation to pulmonary circulation Pulmonary artery thrombus Clots that form in the pulmonary vasculature ID: 1009407
Download Presentation The PPT/PDF document "Pulmonary Thromboembolism" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


1. Pulmonary ThromboembolismBy Dr.Salauddin
2. Pulmonary thromboembolismOne clot or many clots that migrate from systemic circulation to pulmonary circulation.Pulmonary artery thrombusClots that form in the pulmonary vasculature.Clots can partially or fully occlude pulmonary vessels.Definition
3. Embolism : Impaction of a thrombus or foreign matter in the pulmonary vascular bed.Infarction : The pathological changes which develop in the lung as a result of pulmonary embolism.Pulmonary Embolism, Infarction
4. Venous stasis.Injury or abnormalities to the vessel wall.Alterations in coagulation properties.Virchow’s Triad
5. Accumlation of activated procoagulants.ImmobilizationInadequate cardiac pump.Promotes thrombus formation.Venous Stasis
6. Acute or chronic injury to vessel endothelium.Leads to activation of platelets and clotting cascade.Promotes thrombus formation.Vessel Wall Injury
7. Vessel Injury
8. Platelet Adhesion
9. Aggregation
10.
11. Increase in procoagulant factors.By trauma to vascular wall or extravascular tissues.Releases tissue thromboplastin and phospholipid.Leads to formation of prothrombin activator.Prothrombin ThrombinAlternations in Coagulation
12. Decrease in anticoagulant factors.ThrombomodulinAntithrombin IIIHeparinAlpha2-MarcoglobulinPlasminLeads to hypercoagulable state by formation of thrombin.Alterations in Coagulation
13. Platelet nidus at site of injury.Growth by aggregation of platelets and fibrin.Activation of clotting cascade.Larger growth to a red fibrin thrombus.Thrombus fractures and embolizes to other areas of the body.Thrombosis Formation
14. Hypercoagulable stateNephrotic syndrome ,malignancy ,PNHImmobilization,estrogen therapyAmyloidosis,protien C and S deficiencyEarly DICHyperadrenocorticismCapillary fragilityActivation of clotting cascade.Predisposing Factors or Diseases for Development of PTE
15. Hypercoagulable stateCapillary fragilityDiabetes MellitusImmune–mediated hemolyitc anemiaSepsisHyperadrenocorticismActivation of clotting cascade.Predisposing Factors or Diseases for Development of PTE
16. Hypercoagulable stateCapillary fragilityActivation of clotting cascade.SepsisPneumonia/pyothoraxHeartworm diseaseSurgeryBacterial endocarditisNeoplasiaPredisposing Factors or Diseases for Development of PTE
17. Respiratory.Increased alveolar dead space.Hyperventilation.Hypoxemia.Ventilation/perfusion inequality.Intrapulmonary shunts.Consequences of PTE
18. Normal Alveolus
19. Increased Alveolar Dead Space
20. Results from ventilation-perfusion inequality, physiologic shunting and increased dead space. Hypoxemia
21. Blood that has not been to areas of ventilated lung and enters systemic circulation without gas exchange taking place. Poorly oxygenated blood enters the arterial system lowering the PaO2.Not responsive to oxygen therapy.Intrapulmonary Shunts
22. V/Q inequality occurs when distribution of blood is altered to the alveoli.O2 increase in the alveoli and CO2 decreases.Ventilation/Perfusion Inequality
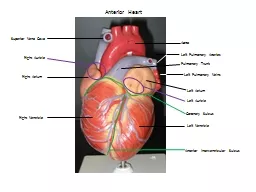
23. Increase in pulmonary vascular resistance.Increased afterload to the right heart.Can lead to circulatory collapse and shock.Hemodynamic Changes
24. Not pathognomonic.Dyspnea.Tachypnea.Hemoptysis.Tachycardia.Hypoxemia.Sudden death. Clinical Signs
25. Clinical Features of PTESilentAsymptomaticProbably more frequent than we realizeWithout InfarctionBreathlessness, Tachycardia, Anxiety, RestlessnessUsually Transient
26. Clinical Features of PTEWith Infarction Dyspnea, Hemoptysis, Pleutitic Pain, Friction Rub, Fever, Brochospasm.If you wait for these features, you will miss perhaps 60% of patients with embolism
27. Clinical Features of PTEWith Hemodynamic ImpairmentAngina, Tachycardia, P++, Gallop, JVP++, Hypotension, Cyanosis, SyncopeThis means obstruction of 30-50% of pulmonary vascular bed
28. Value of Diagnostic Tests in PTEChest X-RayElevated Diaphragm, Wedge-shaped opacity, Atelectasis, Pleural Effusion It may be Normal after acute PEECGSinus Tachycardia, S1, Q3, T3, Rt. Axis P-Pulmonale, Incomplete RBBB , ArrhythmiasChest X-Ray and ECG should be Routine
29. Value of Diagnostic Tests in PTEIsoenzyme PatternNormalOnly helpful in distinguishing PE from MILeucocytic CountUnder 15 000If over 15 000, consider Bacterial Sepsis
30. Value of Diagnostic Tests in PTEArterial Blood Gases ( ABG )Hypoxemia, HypocapniaNon-specificAlveolar-Arterial Oxygen Tension DifferenceIncreased DifferenceMore Sensitive but Non-specific .
31. Value of Diagnostic Tests in PTERadioactive ScanningAbnormal Lung Perfusion with Normal Ventilation . High, Intermediate and Low Probability .Non-specific, Too many False-positive . A Normal Perfusion Scan with a Normal CXR rules out PE .
32. Value of Diagnostic Tests in PTEPulmonary AngiogramIntravacular Filling Defect or Vessel Cut-offThe Most Reliable but InvasiveD-DimersA Good Negative Predictive TestElevated in DIC, Pregnancy, Severe Infection, Trauma, Malignancy, Surgery, Liver Disease
33. Value of Diagnostic Tests in PTESpiral Computed TomographyComparable to Angiography.Cases with Ventilation-Perfusion scan of Intermediate ProbabilityPoor Quality may be obtained as a result of motion artifacts. Clinical AssessmentClinical Scoring Plus ECG, Radiographic Findings, Perfusion Scan.This may restrict the need for Angiography to a minority.
34. High Probability ( 90% ): Presence of at least one of three symptoms ( Sudden onset Dyspnea, Chest Pain, or Fainting ) not explained otherwise and associated with : (1) Any two of the following abnormalities: ECG signs of RV overload, Radiographic signs of Oligemia, Amputation of hilar artety, or Pulmonary consolidations compatible with infarction; (2) Any one of the above three radiographic abnormalities.Clinical Probability of PE
35. Intermediate Probability (50%): Presence of one of the above symptoms, not explained otherwise, but not associated with the above ECG and Radiographic abnormalities, or associated with ECG signs of RV overload only.Clinical Probability of PE
36. Low Probability (10%): Absence of the above three symptoms, or idetification of an alternative diagnosis that may account for their presence (e.g.,exacerbation of COPD, Pneumonia, Lung Edema, Pneumothorax, Myocardial Infarction, and others).Clinical Probability of PE
37. Low Probability (10%): Absence of the above three symptoms, or idetification of an alternative diagnosis that may account for their presence (e.g.,exacerbation of COPD, Pneumonia, Lung Edema, Pneumothorax, Myocardial Infarction, and others).Clinical Probability of PE
38. LaRue MJ and Murtaugh RJ. Pulmonary Thromboembolism in Dogs:47 cases (1986-87). J Amer Vet Med Assoc. 1990 Nov. 15;197(1):1368-1372.Johnson LR et al. Pulmonary Thromboembolism in 29 dogs:1985-1995 J Vet Intern Med. 1999 Jul;13(4):338-345.Flükiger MA and Gomez JA. Radiographic Findings in Dogs with Spontaneous Pulmonary Thrombosis or Embolism. Veterinary Radiology, Vol.25,No.3 124-131.
39. Pulmonary scintigraphy Pulmonary angiography.Advanced Diagnostics
40. NoninvasiveAids in diagnosis of PTE but not definitive.Two types- ventilation and perfusion scans.Pulmonary Scintigraphy
41. Performed first.Normal study rules out PTE.Radionuclide-labelled, macroaggregated albumin in peripheral vein.Perfusion Scan
42. Inhaled radioactive inert gas-senon-133 or technetium-99m.Patient under general anesthesia.Normal in PTE.Ventilation Scan
43. With PTE the ventilation scan would be normal and the perfusion scan abnormal.Suggestive of PTE.FPicture from WWW.bschsys.org/DiagnositcImaging/nucmd/htmVentilation/Perfusion Combo
44. Normal Human Perfusion Scan
45. Abnormal Human Perfusion Scan
46. A Normal Ventilation-Perfusion Scan Excludes Pulmonary Embolism
47. The Combination of A High-Probability Ventilation-Perfusion Scan Plus A High Clinical Suspicion is Diagnostic for Pulmonary Embolism.
48. A Low-Probability or Normal Lung Scan with a Low Clinical Suspicion makes the diagnosis of Pulmonary Embolism Unlikely
49. Performed if definitive diagnosis or exclusion of PTE is required.Requires sedation or general anesthesia.Greater risks.Intraluminal filling defect and sharp cutoff are diagnostic for PTE.Pulmonary Angiography
50. Human lung.Arrow indicates abrupt termination of a pulmonary artery.Www.brighamrad.Harvard.edu/cases/bwh/images.Pulmonary Embolus
51. Pulmonary Embolism, PreventionPatients at risk: Early Ambulation.Risk Factors.During Operations.Prophylactic Heparin.Vein Ligation.Filters.
52. Pulmonary Embolism, Active TreatmentEmbolectomy.Recombinant tissue-plasminogen activator, t-PA.Streptokinase and Urokinase.
53. Pulmonary Embolism, Active TreatmentHeparin, Low-Molecular-Weight Heparin.Oral Anticoagulants.Filters, Vein Ligation.Adjuvants: Oxygen, Antibiotics, Rest in bed.
54. Streptokinase600 000 U in 1/2 h, Then 100 000 U/h for 72h.Thrombin clotting time.EACA: Local and Systemic, Fresh Blood, and Fresh Frozen Plasma.
55. Heparin5 000 - 10 000 U iv Bolus,Then 1000 - 5000 U/ 24 h, or 20 U/Kg/hPartial Thromboplastin Time ( PTT ).Infusion Pump.Action-increase activity of anti thrombin3.Advantage-shorter 1/2life ,useful when undergoing surgery. Dis adv-repeated blood sampling ,heparin induced thrombocytopenia
56. Low-Molecular-Weight-HeparinGreater Bioavailability.-less binding to plasma protien and endothelial cellsCan be given Subcutaneously.Longer duration of Anticoagulant effect.A fixed dose can be used, PTT monitoring is not necessary.Enoxaparin: 1 mg/kg every 12h. Renal excreation –caution when RFT is deranged
57. Oral AnticoagulantsFor long term managementWarfarin used vitamin k antagonistPrevent carboxylation of coagultion factor II IV IX X.Narrow therapeutic index.INR range 2and 3.Drug interaction –metronidazole,barbiturates ,carbamazepine,amiodarone.Teratogenic potential
58. NON MASSIVETHROMBO EMBOLISM MANAGEMENT THREE PHASE 1-initial phase 2-early maintinance phase 3-long term 2ndry prevention
59.
60. Clotting times- want to maintain PTT at 1.5-2.5 times normal or and ACT at 1.2-1.4 times normal. Serial arterial blood gas analysis.Respiratory rate.Central venous pressure.All other basic monitoring.Monitoring
61. Hemorrhage most common. Not predictable. Protamine therapy indicated with hemorrhage due to heparin.Vitamin K or fresh-frozen plasma in warfarin therapy.Complications Of Therapy