
Page 1 of 2 Format and content have been adapted where available with permission from M oun t Sinai H o spital RUXO Version 10 RUXO ruxolitinib Diagnosis Myelofibrosis Clinical Verification ID: 831343
Download Pdf The PPT/PDF document "Developed by the Drug Formulary Team at ..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Page 1 of 2 Developed by the D
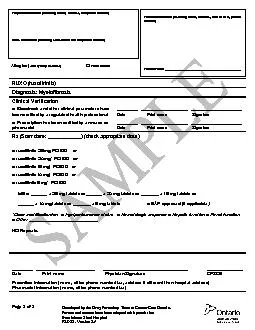
Page 1 of 2 Developed by the Drug Formulary Team at Cancer Care Ontario. Format and content have been adapted where available with permission from Mount Sinai Hospital RUXO - Version 1.0 RUXO (ruxolitinib) Diagnosis: Myelofibrosis Clinical Verification □ Bloodwork and other clinical parameters have ________ __________________ ____________________ been verified by a regulated health professional Date Print name Signature □ Prescription has been verified by an nurse or ________ __________________ ____________________ pharmacist Date Print name Signature Rx (Start date: ____________) (check appropriate dose) □ ruxolitinib 25 mg PO BID or □ ruxolitinib 20 mg* PO BID or □ ruxolitinib 15 mg* PO BID or □ ruxolitinib 10 mg* PO BID or □ ruxolitinib 5 mg* PO BID Mitte: ______ x 25 mg tablets or ______ x 20 mg tablets or _______ x 15 mg tablets or ______ x 10 mg tablets or _______ x 5 mg tablets □ EAP approved (if applicable) *Dose modification for: □ Age/performance status □ Hematologic response □ Hepatic function □ Renal function □ Other ___________________________ NO Repeats ________ _______________________ _________________________________ ______________ Date Print name Physician Signature CPSO# Prescriber information (name, office phone number/fax, address if different than hospital address) Pharmacist information (name, office phone number/fax) Hospital Information (including name, address, telephone number) Clinic information (including clinic name and telephone number) Patient information (including name, address, date of birth, phone number) Patient Name _________________________________________ Allergies (also specify reaction) □ None known Page 2 of 2 Developed by the Drug Formulary Team at Cancer Care Ontario. Format and content have been adapted where available with permission from Mount Sinai Hospital RUXO - Version 1.0 OPTIONAL INFORMATION □ Patient has been counseled by an Oncology Pharmacist ____________________ ________________________________ _______________ Print name Signature Date OR □ Requires counseling □ Drug interac
tion assessment Drug-specific in
tion assessment Drug-specific information For the complete information, please refer to the Cancer Care Ontario drug information sheets available at www.cancercare.on.ca/drugformulary ��Page of Developed by the Drug Formulary Team at Cancer Care Ontario. Format and content have been adapted with permission from Mount Sinai Hospital RUXO - Version 1.0 OPTIONAL INFORMATION Patient has been counseled by an Oncology Pharmacist____________________Print name Signature Date Requires counselingDrug interaction assessmentDrug-specific information For the complete information, please refer to the Cancer Care Ontario drug information sheets available at www.cancercare.on.ca/drugformulary ��Page of Developed by the Drug Formulary Team at Cancer Care Ontario. Format and content have been adapted with permission from Mount Sinai Hospital RUXO - Version 1.0 RUXO (ruxolitinib) Diagnosis: Myelofibrosis Clinical Verification Bloodwork and other clinical parameters have________ __________________ ____________________ been verified by a regulated health professional Date Print name Signature Prescription has been verified by an nurse or________ __________________ ____________________ pharmacist Date Print name Signature Rx (Start date: ____________) (check appropriate dose) ruxolitinib 25 mg PO BID orruxolitinib 20 mg* PO BID orruxolitinib 15 mg* PO BID orruxolitinib 10 mg* PO BID orruxolitinib 5 mg* PO BID Mitte: ______ x 25 mg tablets or ______ x 20 mg tablets or _______ x 15 mg tablets or ______ x 10 mg tablets or _______ x 5 mg tablets □EAP approved (if applicable)*Dose modification for: □ Age/performance status □ Hematologic response □ Hepatic function □ Renal function□Other ___________________________NO Repeats ________ _______________________ _________________________________ ______________ Date Print name Physician Signature CPSO# Prescriber information (name, office phone number/fax, address if different than hospital address) Pharmacist information (name, office phone number/fax) Hospital Information (including name, address, telephone number) Clinic information (including clinic name and telephone number) Patient information (including name, address, date of birth, phone number) Patient Name _________________________________________ Allergies (also specify reaction) 一漀渀攀 欀渀漀眀渀