
Stanford Hospital and Clinics April 26 2010 Motion segment VERTEBRAE Carry 7090 of static axial load Vary in cervical thoracic lumbar sacral and coccygeal FACET JOINT Carry 1020 of static axial load ID: 930569
Download Presentation The PPT/PDF document "biomechanics of the spine" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
biomechanics of the spine
Stanford Hospital and Clinics
April 26, 2010
Slide2Motion segment
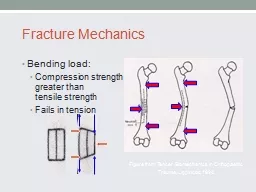
VERTEBRAE
Carry 70-90% of static axial load
Vary in cervical, thoracic, lumbar, sacral and
coccygeal
FACET JOINT
Carry 10-20% of static axial load
Highly innervated and can be a source of low back pain
Cervical spine:
facet orientation is roof-tile shaped, coupling lateral bending and axial rotation in an opposite direction (i.e. bending the head to the left results automatically in an axial rotation to the left
Thoracic spine:
coronal plane orientation with a slight inward tilt in the transverse plane, permitting axial rotation movements with the center of rotation projecting into the vertebral body
Lumbar spine:
sagittal
plane orientation of facet joints, effectively blocking axial rotation movements
Slide3Degree of Facet range of motion
Slide4Motion segment
INTERVERTEBRAL DISC
Nucleus
pulposus
surrounded by annulus
fibrosus
Covers 30-50% of disc surface area and contains exclusively type II collagen fibers in a aqueous gel rich in
proteoglycans
Sharpey
fibers insert from the annulus
fibrosus
into the
epiphyseal
ring
Endplates are composed of a dense layer of
trabecular
bone further covered with a layer of hyaline cartilage
Vascular channels within the vertebral bodies have been observed to run directly along the endplates, representing the predominant nutrient source for adult disc cells
Cartilaginous end plates undergo progressive calcification with age, which impedes nutrition and contribute to the progressive disc degeneration throughout adulthood
Disc degeneration also affects other elements of the motion segment. Through disc height loss and apparent changes in axial load transmission, the facet joints become incongruent and may become mechanically overloaded. Also, loss of disc height will result in ligament laxity,
hypermobility
and loss of segmental stiffness.
Slide5Intradiscal pressure for various activities
Slide6Motion segment
MUSCLES
LIGAMENTS
Slide7SPINAL MOTION
Six degrees of freedom
Motion rarely involve a single degree of freedom only
Segmental Instability
“loss of ability of the spine under physiological loads to maintain its pattern of displacement so that there is no initial or additional neurological deficit, deformity or incapacitating pain.”
- White & Panjabi
Slide8Biomechanics of spinal stabilization
Goals of spinal arthrodesis are:
To support the spine when its structural integrity has been severely compromised
To maintain correction following mechanical straightening of the spine.
To prevent progression of deformity.
To alleviate or eliminate pain by stiffening a region of the spine.
Choose a stabilization method which will best achieve these goals. Therefore, the surgeon needs to have an understanding of how load is transferred
throughout
the spine and how this load transfer is altered by a specific injury or pathology.
Slide9Posterior stabilization
PROVIDES STABILIZATION IN EXTENSION AND LATERAL BENDING
Pullout strength of pedicle screws is directly related to bone density
It is possible to achieve an increase in pullout strength with convergent screw trajectories.
Parallel pedicle screw in short segment constructs can result in an unstable “four bar” mechanism.
Diagonal
cross-linking
is preferable to the horizontal configuration in terms of rotational stability.
An increase in rod diameter provides a more stable construct, but at the same time produces higher internal loads in the implant, on the clamping device, and on the pedicle screws; thus, higher risk of screw breakage.
Slide10Posterior stabilization
Slide11Posterior stabilization
Slide12Posterior stabilization
In the thoracic spine, smaller overall pedicles can result in complications. An alternative is to increase pullout strength with extrapedicular screw trajectory.
Slide13Anterior stabilization
PROVIDES STABILIZATION IN FLEXION AND LATERAL BENDING.
Anterior cervical plates function as tension band during extension and buttress plate during flexion.
Constrained cervical systems have a rigid, angle-stable connection between the plate and screws, whereas, unconstrained systems rely on friction generated by compression of the plate against the anterior cortex for stability.
In extended biomechanical testing, constrained systems have shown a greater rigidity over time, whereas, unconstrained systems can lose stability over time.
No significant difference in stability between monocortical and bicortical screws in the cervical spine.
Slide14INTERVERTEBRAL CAGES
Distraction of facet joints may be associated with instability
Slide15Adjacent segment effects
Fusing
one or two levels will lead to increased stress at the remaining adjacent levels, the remaining motion segments will have to take up and accommodate the remaining motion of the spine, these adjacent levels will then tend to age and degenerate faster because of the resultant increased load and
stress.
Slide16Arthroplasty of the spine
Many
spinal arthroplasty surgeons propose that by performing a disc replacement and restoring motion to a diseased spinal segment, this reconstructed spinal motion segment will offload the stress to the adjacent levels and actually lower the risk of onset of accelerated adjacent segment degeneration. The spine is a mobile structure and motion will occur at the places of least resistance and stiffness, if motion can be restored by a disc replacement then this will lead to reduced stresses at other more degenerated parts of the spine
Slide17“Biomechanical study on the effect of cervical spine fusion on adjacent-level intradiscal pressure and segmental motion”
Eck JC, Humphreys SC, Lim TH, Jeong ST, Kim JG, Hodges SD, An HS. Spine 2002.
Intradiscal pressure and segmental motion are increased in adjacent disc segments after fusion. This cumulatively translates into increased stress on the adjacent non-operated discs, which can accelerate the rate of disc degeneration.
Slide18“Radiculopathy and myelopathy at segments adjacent to site of previous anterior cervical arthrodesis”
Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. J Bone Joint Surg, 1999.
Studied 374 patients and found that symptomatic adjacent segment disease occurred at a relatively constant rate of 2.9% during the decade after surgical fusion.
Slide19Indications and contraindications
Failure in medical management
Normal cervical alignment and mobility with radiculopathy cause by:
soft or hard disc herniation
foraminal osteophytes
myelopathy due to soft disc herniation
Arthroplasty is contraindicated in the setting of significant segmental or global
deformity
Radiographic instability should be treated with
arthrodesis
Recent history of infection or osteomyelitis preclude the use of prosthetic device
Relative contraindications are RA, RF, osteoporosis, cancer, chronic
corticosteroid
use
Marked degenerative changes and no segmental motion cannot be expected to regain mobility by implanting a total disc replacement
Outcomes of patients with isolated axial cervical pain who are treated with an arthroplasty have not been well delineated
Slide20DISC ARTHROPLASTY
Artificial
discs
approved
by the FDA for
use:
Charite
by DePuy
for use in the lumbar
spine
ProDisc
by Synthes
for use in the lumbar spine and cervical
spine
Prestige
by Medtronics for
use in the cervical
spine
Bryan Disc
by Medtronics for use in the cervical spine
These are
FDA approved for one-level applications, after clinical trials showed patient improvement in motion and pain equivalent to spinal fusion.
Two
-level disc replacement surgery is considered experimental in the United States, but has been performed in Europe for many years.
S
ome
insurance companies in the United States do not cover the surgery, still classifying it as experimental.
Effective
August 14, 2007, the Centers for Medicare & Medicaid Services (CMS) will not cover Lumbar Artificial Disc Replacement (LADR) for patients over the age of 60, on a national basis. Individual localities regulate the use of the procedure in patients 60 and under.
Slide21Prestige® ST Cervical disc
Became available in 2002
Constructed of stainless steel in a two-piece ball and trough configuration and attaches to the vertebrae with screws
Provides relatively unconstrained motion comparable to that of a normal cervical spinal segment
Angulation between the base and anterior portion matches the normal anatomy of cervical vertebrae
The surfaces of the device contacting the endplates are grit-blasted to promote bone osteointegration.
Slide22Prestige® LP Cervical disc
Manufactured from a unique titanium ceramic composite material that is highly durable and CT/MRI compatible
Ball and trough configuration is identical to Prestige ST
Initial fixation is achieved via four rails, two on each component
A porous titanium plasma-spray coating on the endplate surface facilitates bone ingrowth and long-term fixation
Slide23Bryan cervical Disc
Conceived in the early 1990s by neurosurgeon Vincent Bryan and first implanted in Belgium in 2000 by Dr. Jan Goffin.
Cervical disc replacement designed to allow for motion similar to the normal cervical spine functional unit.
Consists of two titanium alloy shells with a polyurethane nucleus.
The bone implant interface of each shell has applied porous coating to facilitate ingrowth of bone and promote long-term stability.
The nucleus is surrounded with a polyurethane sheath to establish a closed articulation environment.
Sterile saline is injected into this sheath and functions as an initial lubricant.
Titanium alloy seal plugs allow for retention of the saline lubricant
Small anterior flanges on the shells serve to grasp the device for insertion.
Slide24Prodisc-C cervical disc
Similar design principles as the Prodisc lumbar prosthesis.
First implantation was in December 2002.
Metal-on-polyethylene articulating device consisting of two cobalt-chromium molybdenum endplates and ultra high molecular weight polyethylene inlay.
The endplates are initially secured to the vertebral body with central keels and have a plasma sprayed titanium coating for long-term fixation stability.
Slide25Pcm (Porous Coated Motion) Prosthesis
Made by Cervitech Inc, Rockaway, NJ.
Uses metal on polyethylene articulating surface
The cobalt-chromium-molybdenum alloy components are covered with a TiCaP porous coating
Immediate fixation is achieved by inserting the prosthesis in a “press-fit” fashion.
Slide26Kineflex C Prosthetic Device
Developed in Africa and manufactured by Spinal Motion, Inc, Mountain View, CA
Uses a three-piece modular design consisting of two-cobalt-chromium-molybdenum endplates and a mobile core.
Opposing sides of the endplates have a highly polished concave articulating surfaces.
The core is indented at its equator to permit seating within a retention ring which is an integral part of the inferior endplate. This prevents subluxation of the core.
Initial fixation is achieve via central keel and a pyramidal surface.
Endplate are plasma-sprayed.
Slide27Cervicore disc
Total cervical disc replacement by Stryker Spine, Allendale NJ.
Constructed of cobalt-chromium alloy.
Articulation occurs across a pair of saddle-shaped bearing surfaces.
Two fins containing three fixation spikes provide initial stability.
Bony contact surfaces have titanium plasma-sprayed coating.
Slide28Future direction
Some companies are working
to develop products and methodologies to replace only the inner portion of the
disc, referred
to as
disc nucleus
replacement
. These
new techniques would allow for posterior insertion and a potentially shorter surgery with fewer complications.
Recently new artificial discs with innovative designs that incorporate an artificial nucleus to allow shock absorption and a woven fiber annulus for graded variable motion resistance in all directions have been approved in Europe. These next generation implants are designed to reduce the risk of implant migration found with earlier designs. They also should protect against impact injury and facet joint wear.
Slide29Dynamic
stabilization
(
Dynesys
)
Slide30Interspinous process distraction