
20212022 Canadian partnership against cancer Suggested citation Breast Screening in Canada 20212022 Environmental Scan Canadian Partnership Against Cancer 2022 httpswwwpartnershipagainstcancercatopicsbreastcancerscreeningincanada20212022summary ID: 1039613
Download Presentation The PPT/PDF document "Breast Cancer Screening in Canada" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.





1. Breast Cancer Screening in Canada2021/2022Canadian partnership against cancerSuggested citation: Breast Screening in Canada: 2021/2022 Environmental Scan. Canadian Partnership Against Cancer; 2022. https://www.partnershipagainstcancer.ca/topics/breast-cancer-screening-in-canada-2021-2022/summary/
2. SummaryBreast Cancer Screening Pathway
3. Breast cancer screening pathway3
4. Key HighlightsStrategies Being Implemented to Reach the Abnormal Call Rate Target
5. Strategies Being Implemented to Reach the Abnormal Call Rate TargetP/TMin. Reading VolumeDouble ReadingAudit & performance feedbackComparisons with prior mammogramNumber of mammographic viewsMammographic compressionBatch reading of mammogramFellowship training in breast imagingYT--------NT✓ ✓✓ 4✓ NU BC✓ ✓✓✓4 ✓ AB✓✓ (varies by clinics)✓ (intend to explore)✓✓4✓ (intend to explore)✓ (varies by clinics) SK✓✓ (tech supervisors – discrepancies are reviewed by a 2nd rad)✓ (intend to improve)✓✓✓✓ ✓ (some rads not all)MB✓ ✓✓✓4✓✓✓ (some rads not all)ON✓ ✓✓✓4 ✓ (encouraged at the site level)✓ (some rads, not all)QC✓ ✓✓✓ 4 NB✓✓✓✓✓4✓✓ (May vary by screening site) NS✓✓✓✓✓4 ✓✓*PE✓ ✓✓✓✓✓(encouraged at the site level)✓ (some rads not all)NL✓ ✓✓ ✓ NS: * In Nova Scotia, some radiologists have fellowship training in breast imaging.
6. ProgramsProgramsGuidelinesRecruitmentBooking of Mammograms
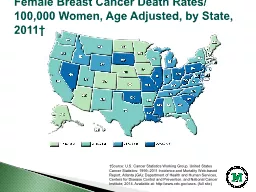
7. 7YukonNorthwest TerritoriesNunavutManitobaSaskatchewanAlbertaBritish ColumbiaOntarioQuebecNewfoundland and LabradorStatus of breast cancer screening programs in CanadaFully implementedNo organized programNew BrunswickNova ScotiaJune 2022PrinceEdwardIsland
8. Breast Cancer Screening Programs in CanadaNT: *Yellowknife Breast Screening Program (YKBSP) and Hay River Breast Screening Program (HRBSP) support 15 of 33 NT communities. The remaining 18 communities that are not part of an organized program book mammograms through the diagnostic imaging department that services their region.P/TProgram start dateProgram nameAgency responsible for program administrationYT1990Yukon Mammography ProgramGovernment of Yukon (Yukon Hospital Corporation)NT*20042008Yellowknife Breast Screening Program (YKBSP)Hay River Breast Screening Program (HRBSP)Northwest Territories Health and Social Services Authority (NTHSSA)Hay River Health and Social Services Authority (HRSSA)NU No organized screening program available BC1988BC Cancer Breast Screening ProgramBC Cancer AB1990Alberta Breast Cancer Screening Program (ABCSP)Alberta Health ServicesSK1990Screening Program for Breast CancerSaskatchewan Cancer AgencyMB1995BreastCheckCancerCare ManitobaON1990Ontario Breast Screening Program (OBSP)Ontario Health (Cancer Care Ontario)QC1998Programme québécois de dépistage du cancer du sein (PQDCS)Ministère de la Santé et des Services sociauxNB1995New Brunswick Breast Cancer Screening Services New Brunswick Cancer Network (NB Department of Health)NS1991Nova Scotia Breast Screening ProgramIWK Health CentrePE1998PEI Breast Screening ProgramHealth PEINL1996Breast Screening Program for Newfoundland and Labrador Cancer Care Program, Eastern Health
9. Provincial and Territorial Screening Guidelines9P/TStart ageIntervalStop ageExclusion criteriaYT50(40 with radiologist recommendation)2 years74Personal history of breast cancerBreast symptomsMammogram of both breast in the last 12 monthsAge <40 yearsPregnant or pregnant in the last 4 monthsBreastfeeding or breastfeeding in the last 4 monthsBreast implantsNT50(40 with referral from PCP)1-2 years74(participants age 75+ have the option to continue, encouraged to speak to their PCP to see if screening is right for them) NUNo organized screening program available BC50(40-49 accepted by self-referral but not actively recruited)2 years74(75+ accepted by self-referral, but not actively recruited)Personal history of breast cancerBreast symptomsBreast implantsAB50(40-49 with PCP referral for first screen)2 years74(75+ with PCP referral to continue screening)Known diagnosis or history of breast cancerBilateral mastectomiesSigns and symptoms which could be associated with breast cancersSK50(49 accepted to mobile unit if turning 50 in the same calendar year)2 years75+Breast cancer in the last 5 yearsSigns and symptoms of breast cancer Breast implantsMB502 years74(75+ have the option to continue)Previous breast cancer diagnosis SymptomaticBreast implantsON502 years74(75+ with referral from PCP) Personal history of breast cancerMastectomyBreast cancer symptomsScreening mammogram within the last 11 monthsBreast implantsQC502 years 69Personal history of breast cancerScreening mammogram within the last 11 months NB50(40 with referral from PCP)2 years74(75+ with referral from PCP)Personal history of breast cancerSymptomatic for breast cancerBreast ImplantsNS50(age 40-49 accepted by self-referral but not actively recruited)2 years74(75+ accepted by self-referral, but not actively recruited)Personal history of breast cancerBreast symptoms Breast implantsPE50(available for age 40-49)2 years74Personal history of breast cancerBreast symptoms Screening mammogram within the last 11 months Breast implantsNL502 years74(age 74+ only if previously enrolled in the program)Personal history of breast cancerBreast symptoms Breast implants
10. Breast Screening Recruitment MethodsNT: * Yellowknife’s BSP accepts self-referrals (50-74) for persons living within the Yellowknife catchment area who have a designated PCP; all other locations they service require a referral from PCP to enter the program. Hay River BSP accepts self-referrals (50-74) for persons living in Hay River catchment with a designated PCP; all other locations they service require a referral from PCP to enter into the BSP. NS: ^ Healthcare provider recommendationP/T Physician referralSelf-referral Initial letter of invitationPromotional Content (e.g., social media, advertisement) Referral from nurse practitioner YT✓✓ NT✓✓* NU✓ ✓BC✓✓ ✓ AB✓✓✓ SK✓✓✓ MB✓✓✓ ON✓✓✓✓✓QC✓✓✓ ✓NB✓✓✓✓ NS✓✓ ✓^PE✓✓ ✓ NL✓✓
11. Booking of MammogramsP/TRole of PCP in access to testBooking screeningScreening locations YTReferral not requiredPerson must identify a PCPPCPs can refer participant and program will mail them their appointment timePerson books by calling program numberFor recall screening, participant can fax in a form they are sent by mail and the program will mail them their appointment timeMammograms available in WhitehorseNo mobile screeningNT Requisition from CHC required to support medical travelPerson must identify PCP when booking appt (program will refer participant to a CHC if they do not have a PCP already)Person books by calling toll-free program numberIndividuals requiring travel support must coordinate the appointment through their CHC· Screening available in Yellowknife for this program (Hay River and Inuvik also offer screening in separate programs)· No mobile screeningNU· Referral from PCP required for out of territory screening.· Screening mammograms need to be coordinated with travel taking place for another reason.None (diagnostic screening only)Limited screening may be done at Qikiqtani General Hospital for individuals who match the following criteria:1. Travelling to Iqaluit for another appointment2. Travelling to Iqaluit as an escort for another patient3. Travelling to Iqaluit for business or leisure4. A referral must be made from a Nunavut licensed physician or NP5. QGH services clients from the Baffin RegionNo mobile screeningBCReferral not requiredMust identify a PCP when booking screening; can be a walk-in clinic, nurse practitioner, or naturopathCall central booking (toll-free) or contact local screening site directlyScreening locations and contact information listed online and available by calling the programMobile screening units availableABReferral not requiredMost screening sites may require PCP be identified when booking mammogram to ensure work upSite assists person to identify a PCP if they do not have oneCall screening site (local number) or mobile units directly to book appointment (participant’s choice)Program does not book appointments centrallyScreening locations and contact information listed online and available by calling the program’s Client Services LineFacility list sent with every invitation and reminder letterMobile screening units availableSKReferral not requiredParticipant encouraged to identify a PCP but can attend appointment without identifying one.Person books by calling toll-free program numberScreening locations and contact information listed online and available by calling the programMobile screening units availableMBReferral not requiredParticipant encouraged to identify a PCP, but can attend appointment while trying to find a PCPPCPs can refer participant for screening. Program will contact person to set up the appointmentCall (toll-free) program (for mobile and fixed sites)Screening locations and contact information listed online and available by calling the programMobile screening units availableONReferral not required, but PCPs, including nurse practitioners, can refer participantsInitial invitation letters sent to those not currently enrolled in the screening program with details about screening and how to book an appointmentIf referral was sent directly to a site, the site will contact the participant to schedule an appointmentParticipants can book by calling individual screening sitesMobile coaches are linked to specific sites and appointments for mobile coaches are set up through these sitesScreening locations and contact information is available online or by calling the programParticipant’s recall letter also provides the phone number of the screening site where their last screen was completedMobile screening coaches availableQCReferral not requiredPerson books by calling screening site (toll-free or local number)Participant provided with a list of nearby screening sites in their invitation letterMobile screening units availableNBReferral not required; Screening sites accept PCP referrals and then contact person with appointment timeCall closest screening site (mostly local numbers, some toll-free) directly to book appointmentNB Cancer Network of the Department of Health provides a list of all breast screening sites and their contact information on their websitePublic may call the toll-free Cancer Screening line for breast screening clinic contact information.No mobile screeningNSReferral from PCP not requiredParticipants are asked to identify PCP when booking appointment. Program will work with person to identify PCP if they do not have a PCP already.Participant self-refers by calling toll-free program number.They can choose to be screened at any of the breast screening sites (fixed or mobile).There are 11 fixed breast screening sites and 30 mobile stops.Location/address information is available on the NSBSP website, or participants can call the toll-free program number.Mobile screening available.PEReferral by PCP is not requiredParticipant self-refers by calling toll-free program numberTwo screening locationsNo mobile screening availableNLReferral not requiredParticipant can book by calling program (toll-free), or by calling (local number) or visiting a local screening siteFor recall screening, participants are given an appointment date and time with their result letters. A reminder letter of appointment is sent to the individual 4 weeks before upcoming appointment.3 screening centresNo mobile screening
12. 12Modalities for breast screeningPrimary modalities for breast cancer screeningMobile breast screeningOther breast screening modalities
13. Primary Breast Screening Modalities in Canada: Digital Mammography**Digital mammography: mammography images are captured and manipulated electronically and includes digital radiography (DR) and computed radiography (CR) systems NB: ^Province-wide DR mammography as of February 2020P/TDigital radiography (DR)Computed radiography (CR)YT✓ NT✓ NU✓ BC✓ AB✓ SK✓ MB✓ ON✓ QC✓✓NB^ ✓ NS✓ PE✓ NL✓
14. Location where Mammography Screening is ConductedQC: *Private imaging centers where breast screening and diagnostic imaging is funded by the governmentP/THospitalScreening CentrePrivate clinicCommunity clinicMobile unitYT✓ NT✓ NU✓ BC✓ ✓ ✓AB✓ ✓ ✓SK✓✓ ✓MB ✓ ✓ON✓ ✓ ✓QC✓ ✓* ✓NB✓✓ NS✓✓ ✓PE✓ NL ✓
15. Mobile Breast Cancer ScreeningP/TMobile Screening Available? Locations of mobile screeningFrequency of mobile unit availabilityPrimary populations servedYT NT NU BC✓Throughout BC1 – 4 times per depending on area populationRural and remote communities including Indigenous communities, correctional facilities, underserved communitiesAB✓120 communities throughout AlbertaRotation schedules of 1-2 yearsRural and remote communities; Indigenous; underservedSK✓~40 sitesEvery 2 years it attends each siteRural, remoteMB✓90 locations across province over a bi-ennial rotation1-2 yearsAll Manitoba participants 50-74 years of ageON✓Two mobile coaches: One travels throughout the North West region and the other travels throughout the Hamilton Niagara Haldimand Brant region in OntarioMobile coaches operate throughout the year and locations can be found: https://www.cancercareontario.ca/en/find-cancer-services/mobile-screening North West: those living in rural and remote settingsHamilton Niagara Haldimand Brant region: people with low income, poorer health outcomes and lack of access to traditional health care primarily in urban settingsQC✓ NB NS✓30 mobile stops; generally beyond 50 km of the closest fixed siteMobile follows a set schedule annually, from March to NovemberFirst Nations, African Nova Scotians, rural/remote communitiesPE NL
16. 3D Tomosynthesis**Tomosynthesis (also known 3D mammography): emerging technology that allows the breast to be viewed three-dimensionallyP/TUsed for High RiskUsed for Average Risk Use of TomosynthesisPlans to Implement TomosynthesisYT ✓Used on all screening exams since December 2020 NT ✓NU 2D Tomosynthesis used at QGH BC✓(research setting only) Only used at two sites that are participating in national TMIST trial AB✓✓Tomosynthesis used widely with some sites on every screen and others on dense breasts only. Province has modifier billing code. SK Currently used in some diagnostic settings throughout the province.✓ (with equipment upgrades throughout the province)MB ON Not currently recommended. However, for sites with digital breast tomosynthesis, this technology can be used as part of breast assessments. If digital breast tomosynthesis is being offered to Ontario Breast Screening Program (OBSP) participants for screening purposes, then it must be done and reported outside of the program after the OBSP two-dimensional views have been obtained. No plan to implement tomosynthesis, but Ontario Health (Cancer Care Ontario) continues to monitor the evidence. QC Not recommended for screening. Used in diagnostic imaging according to INESSS recommendations. NB Not recommended for screening. Used by some sites as supplemental investigations for individuals with dense breasts. Currently available at 2 sites.Under evaluation as part of current Increased /High Risk Guideline development.NS Not used in breast screeningNo plans to implement tomosynthesis PE ✓Plans to purchase tomosynthesis as replacement equipment within next yearNL ✓(Tomosynthesis is being considered when equipment is due for replacement in 2022).
17. MRI and UltrasoundNU: ^Ultrasound is used on all patients under 35.P/TUse of MRI in High RiskUse of MRI in Average RiskUse of Ultrasound in High RiskUse of Ultrasound in Average Risk YT NT NU ✓^BC AB✓ ✓(Some sites use as supplemental for dense breasts or if patient cannot tolerate MRI) SK✓ MB ON✓ ✓(if MRI is not medically appropriate) QC NBUnder evaluation as part of current Increased /High Risk Guideline development Under evaluation as part of current Increased /High Risk Guideline development NS✓ PE✓ NL
18. 18Correspondence and follow-up strategiesFollow-up after a normal mammogramFollow-up after an abnormal mammogram
19. Receiving Results and Follow-Up for Normal Breast Screening Test ResultsNU: * For screens done out of territory, would follow out of territory jurisdictional protocolsP/TMailed to participantSent to PCP/ healthcare providerYT✓✓NT✓ NU* ✓(varies by site)BC✓✓AB✓ SK✓✓MB✓✓ON✓✓QC✓✓NB✓ ✓NS✓✓PE✓✓NL✓✓
20. Recall Methods for Normal Breast Screening Test ResultsNU: * For screens done out of territory, would follow out of territory jurisdictional protocolsP/TRecall mailedPhone call Process varies by siteNo formal recallYT✓✓ NT✓✓ NU* ✓BC✓✓ AB✓ SK✓ MB✓ ON✓ QC✓ NB ✓✓(phone call or letters) NS✓ PE✓ NL✓
21. Recall Interval for Normal Breast Screening ResultsNU: * For screens done out of territory, would follow out of territory jurisdictional protocolsON: ^In Ontario, most participants are recalled every 2 years; however, some participants are recalled in one year based on identified risk factors and/or radiologist recommendation.P/T1 – 2 years2 yearsOr based on radiologist recommendationOr based on identified risk factorsYT✓✓✓✓NT ✓✓✓NU* BC✓ ✓AB ✓✓ SK ✓✓✓MB ✓✓✓ON ✓^ QC ✓✓✓NB ✓✓✓NS ✓✓ PE ✓✓✓NL✓ ✓✓
22. Breast Screening Reminder NotificationsP/TReminder notificationsYTNoneNTReminder letter sent to patient 2 weeks before the beginning of the month screening is due, second reminder letter sent 15 days after appointment is due if patient has not been seen or booked for a mammogramNUNo organized screening program availableBCA series of up to 3 postcards are sent over a 23-month period as reminder notificationsABReminder letter is sent from the program once when >120 days overdueSKReminder letter sent 2 weeks after initial invite if no appointment is booked.MBReminder letter is sent 3 weeks after the invitation/recall letter if an appointment is not scheduled. If continued no response, a recall letter will be sent annually until response or participant ages out (75) of program. A maximum of 4 sets of letters (invitation, recall, and reminder) will be sent.ONRecall reminder letter sent by screening program approximately 10 weeks after the recall letter if screening is not initiated QCRecall reminder letter sent by screening program approximately 10 weeks after the recall letter if screening is not initiatedNBNoneNSReminder postcards are sent 3 months prior to the individual’s due date if screening appointment has not been scheduled. Email reminders are currently being explored.PEReminder letter sent 5 months prior to individual’s due date with an overdue letter 2 months following the person’s due date if screening is not initiatedNLAppointment reminder letter sent to participant 4 weeks prior to scheduled appointment. If a person books or changes their appointment within the 4-week window a reminder letter is not sent. Participants are given their recall appointment to screening when they receive their result letter.
23. Receiving Results and Follow-Up for Abnormal Breast Screening Results (1/2)P/TReceive abnormal resultsFollow up of abnormal resultsLocation of diagnostic mammogram after abnormal resultReturn to screening?YTMailed to individualProgram may also contact participant by phone depending on the follow up required (imaging)Program calls individual to arrange follow up appointments for imagingIf biopsy required, the person must go back to their PCP for referral to biopsy or any other follow upScreening programIf follow up results are normal, participants are recalled for screening every 2 years (or as recommended by radiologist)NTParticipants in the program receive a phone call as well as a letterProgram calls person to arrange follow up appointments for imagingIf biopsy required, the individual must go back to their PCP for referral to biopsyProgram notifies PCP that a patient requires biopsyStanton Territorial Hospital or a facility in Edmonton, AlbertaIf follow up results are normal, participants are recalled for screening every 2 years (or as recommended by radiologist)NUVaries by site; generally sent to PCP who will contact participant to provide resultsPCP manages referrals for any follow up required BCParticipant receives phone call from diagnostic centre to book follow upResults also sent to PCP and mailed to participantDiagnostic Centre books follow up and calls participant with appointmentsAffiliated Diagnostic imaging departmentsIf follow up results are normal, participants are recalled for screening every 1-2 years per identified risk factor program policyABMost clinics notify PCPs and/or participant in person or by phone.Results also sent to PCP and mailed to the individualClinic or PCP contacts person to arrange follow upSome clinics book follow up directly (varies by site)If mammogram was completed at a facility that can do diagnostic mammograms, then usually done at that facilityPrivate clinicsHospital facilitiesIf follow up results are normal, participants are recalled for screening every 2 years (or as recommended by radiologist)SKParticipants receive results by phone, either from program (navigator) or their PCPProgram navigator arranges follow up if given permission to do so by HCP (otherwise HCP will arrange follow up)If program conducting follow up, they contact the participant by phone to arrange appointmentsDiagnostic breast imaging centres (hospitals, private radiology clinics, and/or Breast Health Centres)If follow up results are normal, individuals are recalled for screening every 2 years (or as recommended by radiologist)Individuals who are diagnosed with cancer return to regular screening once they have been cancer-free for five years although currently our software system does not re-invite them. MBParticipants receive phone call from program to provide resultsResults also sent by letter to participants and their healthcare providerReferral to diagnostic centre coordinated by program. Individual is advised of follow up appointment by program (phone).Diagnostic imaging centreIf follow up results are normal, participants are recalled for screening every 2 years (or as recommended by radiologist)All individuals are informed of their status (i.e., if they will be recalled for screening or are no longer eligible) by letter once diagnostic work up is complete
24. Receiving Results and Follow-Up for Abnormal Breast Screening Results (2/2)P/TReceive abnormal resultsFollow up of abnormal resultsLocation of diagnostic mammogram after abnormal resultReturn to screening?ONOBSP sites are expected to ensure that the participant’s PCP is informed of the abnormal breast screen results as soon as possible. Participants’ receipt of abnormal results varies by site: some may call, others send letters, a few may liaise with the PCP who will contact participant to provide results.Follow up varies by site: some sites may coordinate appointments; at other sites the PCP may coordinate follow upIf participant does not have a PCP, the screening site will designate a physician who will manage follow up for the participant until diagnosis Program assessment sites (hospitals and independent health facilities) that conduct diagnostic imagingAssessment sites outside of the program (hospitals and independent health facilities) that conduct diagnostic imaging If follow up results are normal, most participants are recalled for screening every 2 years QCMailed to personPCP or centre will contact participant to provide resultsVaries; participants are directed to contact site or PCP in their results letter, some sites contact the person proactively to arrange follow upDesignated screening centres or reference and diagnostic designated centresIf follow up results are normal, participants are recalled for screening every 2 years (or as recommended by radiologist)NBMost sites contact participant by phoneVaries across sites, participant is typically referred automatically for diagnostic procedureSites vary across zonesParticipants with an abnormal mammogram but no cancer diagnosis can return to the screening program and be re-invited for screening with a physician or nurse practitioner’s recommendationNSMailed to participantResult letter e-faxed to PCP 3 days before letter sent to individual, so that PCP can notify them of their abnormal results and of their follow-up appointment information.Program schedules follow-up appointments per radiologist recommendation; appointment information mailed to PCP and to participant in results letters.Booking process for needle core biopsy varies by site – some booked as per radiologist recommendation (without requisition), others require requisition from PCPDiagnostic breast imaging departments located in hospitalsIf follow-up results are normal, then individuals are recalled for screening every 2 years (or yearly if recommended by radiologist)PENotification of follow up imaging mailed to participant Results letter mailed to PCPNotification through abnormal results letter for follow up appointment Individual is contacted by phone the day prior to appointment If biopsy is required, the PCP contacts the individual Screening program & diagnostics performed at same 2 hospital sitesBiopsy at one site onlyIf follow up results are normal, individuals are recalled for screening every 2 years (or as recommended by radiologist)NLMailed to participant Results mailed to PCP 2 days before individual Program coordinates follow up testing appointments and provides to participants by mail along with abnormal resultsAppointment with PCP may be made but is not requiredDiagnostic breast imaging departments located in hospitalIf follow up results are normal, individuals are recalled for screening every 2 years (or as recommended by radiologist or program protocols)
25. Process When Participants do not have a Primary Care Provider or Cannot be ReachedP/TProcess when participants do not have a PCPProcess when participants cannot be reachedYTPCP Identified when booking the mammogramFollow-up with PCPNTParticipant must have a PCP to be screened. PCP identified when booking the mammogram. YKBSP: Program Booking Coordinator will contact the patient by telephone if further imaging is required. If it is something that cannot be completed in Yellowknife a letter is sent to inform the PCP, who is responsible for the referral. If letter is returned the program will check electronic and hospital systems to confirm address and then call patient to confirm address with them.HRBSP: No specific policy. Program Coordinator will call the patient’s listed phone number if patient is from Hay River or Enterprise, if patient lives in an outlying community a call is placed to the community health centre/PCP. NUPCP identified based on jurisdiction where scan takes place BCParticipant must have a PCP to be screened. PCP Identified at time of booking the mammogram.Follow-up with PCPABPCP usually identified when booking the mammogram. Program will assist participant with finding a PCP either before the screen or after an abnormal result.Screen site will notify PCPSKClient navigator works with participant to find PCP. Program can also refer person to a healthcare provider who will manage follow up.Follow-up with HCP for current phone numberMBProgram will assist participant to obtain a PCP though the provincial ‘Doctor Finder’ initiative in the result of an abnormal result. If a PCP cannot be obtained, Program Medical Lead will assume care of patient for follow up testing.A result letter is mailed to the participant and their PCP (includes a notation thatwe have been unable to reach the participant by phone)ONIf participant does not have a PCP, the screening site will designate a physician who will manage follow up for the participant until diagnosis.Program site will notify PCP and help schedule a follow up appointment. Program site may also continue to call and/or send a letter to the participant, requesting them to follow up with the site.QCVoluntary Program PCP is assigned to the participant to manage follow-upProgram coordinators contacts participant or PCP 45 days (or less) after an abnormal screening test if no supplementary exam has been confirmed in the information system. If participant is still unreachable after 90 days, send registered mail.NBNo official process. Approach varies by site.No official process. Approach varies by site.NSIn the event of an abnormal screening report, the program works with the coordinator of each screening site to get a local PCP in the area to accept the report Central booking site will call the participant. If not successful, central booking staff will contact the PCP to obtain participant’s current contact infoPEProvincial Coordinator (designate), or surgeon contacts the participant about follow-upFollow-up with phone call to PCPNLProgram will assist participant with finding a PCP but will still screen participant. Medical Director and Cancer Screening Pathway Coordinator work with individual to ensure all follow-up is completeCheck alternate source for address, if more recent address found re-send. Otherwise follow-up with PCP
26. 26Breast screening for individuals at elevated and high riskElevated riskHigh riskBreast density
27. Definitions of Elevated Risk for Breast CancerP/TFirst-degree family historyHormone replacement therapy Breast density > or ≥ 75% History of high-risk benign breast disease Radiologist recommendationsOtherYT✓ ✓* ✓ NT✓✓✓✓✓Above average exposure to estrogen Drinking more than one drink of alcohol per dayBeing overweight or obese after menopauseSmoking, especially if started at a young age and before the birth of first child. NU✓ ✓ BC✓ ✓ AB✓ ✓✓✓ SK✓✓✓✓✓Personal history of breast cancerPersonal history of other cancerMB✓ ✓✓At least one 1st or 2nd degree female relative on either maternal or paternal side of the family with a history of breast or ovarian cancer that does not fall into the high increased risk categoryAshkenazi decentON✓ ✓✓✓Personal or first-degree family history of ovarian cancerFirst-degree male relative with breast cancer at any ageTwo or more first-degree female relatives with breast cancer at any age, or one under age 50QC Does not classify participants as high riskNB Under evaluation as part of current Increased /High Risk Guideline development.NS✓✓ ✓✓ PE✓ ✓✓✓ NL✓ ✓✓ Participants with four second degree relatives on the same side of the family (grandparent, aunt, uncle, niece, nephew, half sibling with breast or ovarian cancer)Participants with three second degree relatives with breast or ovarian cancer on the same side of the family with one or more of the following:One person affected < 50 years of ageBreast and ovarian cancer in the same individualMale breast cancerParticipants with a personal history of ovarian cancer diagnosed < 50 years of ageParticipants who have received mediastinal radiation before 30 years of ageParticipants who have been assessed by genetics and confirmed to be at a high risk of breast cancerYT: * Applies to participants who receive a ‘D’ breast density score (BI-RADs category D- extremely dense >75% glandular)
28. Management of Participants at Elevated Risk by Screening ProgramsAB: *The ABCSP does not have official recommendations for elevated risk as the program includes all eligible individuals; however, PCPs and radiologists can make screening recommendations based on individual risks.ON: ^ The OBSP does not use the term “elevated risk”, however, there are several reasons a participant in the OBSP will be recalled by the program in one year: documented pathology of high risk lesions; a personal history of ovarian cancer; two or more first-degree female relatives with breast cancer at any age; one first-degree female relative with breast cancer under age 50; one first-degree relative with ovarian cancer at any age; one male relative with breast cancer at any age; breast density ≥75 percent at the time of screening; or recommendation by the radiologist at the time of screening or assessment.NB: ~Provincial recommendations for those assessed at Increased or High Risk of developing breast cancer are currently under development. NB does not plan to use the term elevated risk.PE: ** Participants with a first degree relative with a history of breast cancer can enter the screening program at an earlier age with documentationNL: ‡ Start/stop age is variable depending on conditions for elevated risk designation (e.g. breast density ≥75% may be a transitory condition, therefore start/stop age would be adjusted)- No information was provided at the time the data were collected.P/TDoes the program manage participants who are at elevated risk? (✓)Recommended screening modalityRecommended start ageRecommended intervalRecommended stop age YT✓MammographyNone givenAnnualNone givenNT✓YKBSP: mammography and ultrasound, MRI in some casesHRBSP: mammography40(40 with referral from PCP, 50 self-referral)1-2 years, based on radiologist recommendation74(75+ have the option to continue screening)NU-----BC✓Mammography40Annual for those with family history or history of benign high-risk breast lesions74AB*-----SK✓Mammography40 (with referral from PCP to diagnostic centre, 50 self-referral)Annual for those with family history and high breast density, history of benign high-risk breast lesions74(75+ have the option to continue screening)MB✓Mammography50Varies depending on level of risk and radiologist recommendation74(75+ have the option to continue screening)ON^✓Mammography50Ongoing annual screening for those with family history and/or documented pathology of high-risk lesionsTemporary annual screening for those with breast density ≥75% at the time of screening or based on recommendation by the radiologist at the time of screening or assessment 74QC-----NB~-----NS✓Mammography50 (40-49 can self-refer)Annual74PE✓**Mammography50 (40-49 can self-refer)Annual74NL✓Mammography50‡ Annual74~
29. Definitions of High Risk for Breast CancerON: *The High Risk Ontario Breast Screening Program (OBSP) does not accept new participants over age 70. However, when participants already in the High Risk OBSP turn 70, the program will continue to screen them with only mammography every year until they are age 74.Abbreviations: Atypical Ductal Hyperplasia (ADH)^, Atypical Lobular Hyperplasia (ALH)^, and Lobular Carcinoma in Situ (LCIS)~^ https://www.cancer.org/cancer/breast-cancer/non-cancerous-breast-conditions/hyperplasia-of-the-breast-ductal-or-lobular.html ~ https://www.cancer.org/cancer/breast-cancer/non-cancerous-breast-conditions/lobular-carcinoma-in-situ.html P/TKnown carrier of a deleterious gene mutation (e.g. BRCA1, BRCA2) First-degree relative of a mutation carrier (e.g. BRCA1, BRCA2) and have declined genetic testingAt ≥ 25% lifetime risk of breast cancer (assessed using IBIS or BOADICEA/ CanRisk risk assessment tool) Received chest radiation before age 30 and at least 8 years previously OtherYT Does not classify participants as high riskNT✓✓ ✓Confirmed mutations of BRCA1 or BRCA2 genesRadiation treatment to chest areaFirst degree family history of breast cancerPersonal or first degree family history of ovarian cancerHighly dense breast tissue (Greater or equal to 75% as shown on mammogram)Personal history of breast biopsies showing Atypical Ductal HyperplasiaNU Patient who has had breast cancer1st line relativePatient is symptomaticBC✓✓✓✓Very strong family history of breast cancer: 2 cases of breast cancer in close female relatives on the same side of the family, both diagnosed before age 30, or 3 or more cases of breast cancer in close female relatives on the same side of the family, with at least one diagnosed before age 50AB✓✓✓✓Ashkenazi decentADH, ALH, LCISSK✓✓✓✓Radiologist recommendationBreast density ADH, ALH, LCISphysician/radiologist requestMB✓ The ‘Claus model’ of risk assessmentAshkenazi decentADH, ALH, LCISON✓✓✓✓Ages 30-74 *No breast cancer symptoms Deleterious gene mutations that confer higher risk of breast cancer (e.g., TP53, PTEN, CDH1)QC Does not classify participants as high riskNB Under evaluation as part of current Increased /High Risk Guideline development NS✓✓✓✓ PE✓✓✓✓ NL✓✓ ✓
30. Management of Participants at High-Risk by Screening Programs P/TDoes the program manage participants who are high risk? How are high risk participants managed?Recommended screening modalityRecommended start ageRecommended intervalRecommended Stop age YT NT✓Mammography only other modalities managed by PCPYKBSP: mammography and ultrasound; MRI in some casesHRBSP: mammography40Based on radiologist recommendation74NU✓Referred to diagnostic centre MammographyVariesBC Eligible for annual routine screening, but no supplemental screening, referred to high risk clinicMammography40Annual74AB Managed by PCP or high risk clinicsMammography & screening breast MRINo earlier than 25 and no later than 40Annual74SK Managed by PCP referral to High Risk Screening programN/AN/AN/AN/AMB Eligible for annual routine screeningMammography50Annual (can vary)Or as per radiologist recommendations74(75+ have option to continue screeningON*✓Referred to the High Risk OBSP by physician Once enrolled in the High Risk OBSP, the participant’s High Risk OBSP site manages their initial and subsequent screenings and communication of results. 30-69: Mammography and MRI (or ultrasound if MRI is not medically appropriate)70-74: Mammography only 30 Annual 74 QC NB Currently managed by radiologistUnder evaluation as part of current Increased /High Risk Guideline developmentUnder evaluation as part of current Increased /High Risk Guideline development Under evaluation as part of current Increased /High Risk Guideline developmentUnder evaluation as part of current Increased /High Risk Guideline developmentNS~✓Eligible for annual screening mammography and screening breast MRI. Annual requisitions for MRI no longer required. High risk patients will be managed similar to average risk clients. Screening Mammography and MRI spaced 30 days apart30Annual74PE✓Annual screening(referral from PCP is required)Mammography and MRI40 (or as recommended by a radiologist)Annual74NL Eligible for annual routine screening, but no supplemental screening, PCP may order supplemental testing – MRION: *Participants must have no breast cancer symptoms and require a valid Ontario Health Insurance Plan number and confirmed high risk status based on program criteria to participate in the High Risk Ontario Breast Screening Program (OBSP). The High Risk OBSP does not accept new participants over age 70. However, when participants already in the High Risk OBSP turn 70, the program will continue to screen them with only mammography every year until they are age 74.NS: ^Nova Scotia Breast Screening Program’s high-risk screening clinical practice guideline has been approved.
31. Definition and Data Collection for High Breast Density by Screening ProgramsYK, BC, MB, NB: * Breast Imaging and Reporting Data System (BI-RADS) categories for breast density: A- almost entirely fatty (<25% glandular); B- scattered fibroglandular densities (25-50% glandular); C- heterogeneously dense (51-75% glandular); D- extremely dense (>75% glandular).BC: ^ BC radiologists categorize breast composition using BI-RADS to assess the volume of breast density. The C and D categories are commonly referred to as “dense”. BC Breast Screening currently provides BI-RADS assessment for participants and providers; however, it has no definition for “high breast density”.P/TDefinition of high breast densityDoes the program collect information on breast density?Does the program recommend more frequent screening for those with high breast density? YTBI-RADS* category D✓✓NT≥ 75% glandular tissue✓✓NU ✓BCBI-RADS*^✓ AB≥ 75% glandular tissue✓ SK≥ 75% glandular tissue✓✓MBBI-RADS* category D✓ ON≥ 75% fibroglandular tissue✓✓ (recalled in 1 year instead of 2 years)QC≥ 75% glandular tissue✓ NBBI-RADS* classification C (heterogeneously dense) or D (extremely dense)✓ (the Program’s legacy database is currently unable to collect this new BIRADS classification data set; Historical data of categories as < or > 50%; data is what is available)Recommendations for the management of High Breast Density are under development as part of Increased/High Risk CPGs; Currently supplemental screening is based on Radiologist recommendationsNSCategory C (heterogeneously dense) or Category D: (extremely dense)✓Radiologist can recommend more frequent breast screening.PE≥ 75% glandular tissue✓✓NL≥ 75% glandular tissue✓✓
32. Notification of Participant’s Breast DensitySK: *Informed that they have dense breasts, but not informed what their dense percentage isP/TAre participants notified of their breast density? If participants are not notified of their breast density, are there any plans to send out notifications?YTNo(Participants can request information from their PCP; all screening reports include density information)Not at this time – working on a plan to implement thisNTNo(Documented on mammogram report to PCP but not included on results letter received by participants)Intend to exploreNU BCYes(They receive their BI-RADS breast density assessment with their results and an informational brochure) ABYes(Participants receive their BI-RADS breast density assessment with their results; additional information may be provided in pamphlet or accessed online) SKYes* (Approximately one week after their mammogram they receive a letter informing them that they have breast density along with a recommendation to screen annually and an information leaflet about breast density)Program is working on how to implement standardized reporting throughout screening and diagnostic settings.MBYesThey receive their BI-RADS breast density assessment with their results and an informational brochure) ONYes Participants with≥ 75% fibroglandular tissue receive a screening result letter accompanied by a breast density fact sheet. The letter informs the participant that their next mammogram should be in one year due to dense breast tissue as seen on their mammogram. In April 2020, the OBSP launched the Breast Density Notification project to ensure OBSP participants can access their Breast Imaging Reporting and Data System (BI-RADS) breast density classification, and develop evidence-informed educational materials and communications to support enhanced breast density notification. The recently updated OBSP Screening Report form requires radiologists to report both a percentage mammographic density and BI-RADS breast density category. All OBSP participants’ PCPs receive both breast density measurements. The two-year normal result letter has also recently been updated to inform participants that they can access their breast density information from their family doctor, nurse practitioner or the OBSP site where their mammogram was performedQCNo(PCP receives report with breast density. PCP can inform the patient.)NoNBYesParticipants are notified of their breast density (BI-RADS category) in their screening results letter, accompanied by a breast density info sheet) NSYes(Participants are notified of their breast density (BI-RADS category) in their screening results letter, accompanied by a breast density fact sheet) PEYesAs of Jan 2020, participants receive a screening result letter with their breast density indicated and a density fact sheet. Prior to this, the PCP was notified of breast density information NLYes(Patient are told in results letter that MBD is greater than 75% or less than or equal to 75%
33. 33Population Outreach All eligible peopleFirst Nations, Inuit, and Métis Underserved populationsRural and remote populationsLGBTQ2S+
34. Strategies to Improve Breast Screening for All Eligible People (1/2)P/TStrategies used Description of activities to improve breast screening for all eligible peopleNTEducation Media (small and mass)Client reminderRecall systemPatient navigationHealthcare provider cultural competency trainingBreast Cancer Screening awareness kits were developed and distributed to all community health centresSocial media posts created and launched on the Northwest Territories Health and Social Services social media platforms (Twitter, Facebook, instagram) Reminder letters mailed to patientsRecall systems for patients in place1:1 health education available with HCP’s in primary care clinics and community health centresBCHealth care provider educationPatient reminder lettersProvider-to-patient letters for overdue patientsProvider recall and result systemsAnnual provider report cards Traditional mediaDigital engagement and social mediaWebsiteSuite of printed resources for patients and providersTranslated and culturally relevant materials and resourcesBroad campaigns and awareness monthsPatient testimonial videosAnimated patient education videosAdvertising (Online, Radio, TV) BC Cancer Breast Screening employs a comprehensive approach to health promotion, including the engagement of health care providers in supporting patient education and navigation of screening pathway. The program provides screening information to patients in diverse ways, from printed resources to digital engagements, while considering their place in the screening journey, from initial awareness to long term participation in the program. ABEducation (one on one and group)Client invitation and remindersMedia (small and mass)Provider assessment and feedbackMobile screening clinicsHealthcare provider cultural competency trainingDevelopment of culturally safe materials and resourcesProgram developed materials are in plain language.Share evidence and learnings with service providers to provide culturally safe care. Inclusive language in Standards and Guidelines. Work with our partners to provide consistent messaging to eligible people. Work with partners to provide providers with their annual panel reports on screening. Ongoing communication about screening through profession associations and colleges. SKEducationRemindersMedia campaignsRecall systemMobile unitPatient navigationHiring outreach manager to develop strategies and a team to target populations with low screening ratesMBComprehensive letter campaignsInformative web siteTV advertisement (run at select periods)Satisfaction surveysAccessibility - 2 mobile clinics, 4 fixed locationsSocial media promoting mobile clinicsInvitation letters sent to all new 50-year-olds and new ManitobansReminder and recall letters sent at appropriate intervalsScreening Program web page on CCMB site that educates and provides for test requestsTV ad runs in October. Promotional pieces in development that support tv adSatisfaction survey sent to all clients testing positive who have gone on to have follow up investigationInteractive map showing active mammogram clinics https://www.cancercare.mb.ca/screening/breast
35. Strategies to Improve Breast Screening for All Eligible People (2/2)P/TStrategies used Description of activities to improve breast screening for all eligible peopleONMass media (small and mass)Development of culturally safe materials and resourcesCorrespondence campaigns (invitation, recall and reminder letters)Provider reminder and recall systems (Screening Activity Reports)Provider incentive strategiesParticipant navigationMass media (small and mass) and development of culturally safe materials and resources: Ontario Health (Cancer Care Ontario) has a Breast Cancer Awareness Month (BCAM) campaign each October. The campaign includes the development and dissemination of promotional materials to regions. These materials include images which are representative of diverse groups.The Ontario’s Ministry of Health will be leading a public campaign to remind people about the importance of regular cancer screening in September 2021 and have provided Ontario Health (Cancer Care Ontario) with support to develop additional strategies to support COVID-19 recoveryCorrespondence campaigns (invitation, recall, and reminder letters): The Ontario Breast Screening Program sends letters to eligible people inviting them to participate in screening by talking to their PCP and reminding them when it is time for their next screening test (recall letter). Provider reminder and recall systems (Screening Activity Reports): Ontario Health (Cancer Care Ontario) helps PCPs identify people eligible for screening or follow-up through the Screening Activity Report, an online tool that gives physicians who participate in Patient Enrolment Model practices the screening status of each of their enrolled age eligible patients (i.e., those who are overdue, never been screened or require follow up).Provider incentive strategies: To support family doctors in ensuring that their patients participate in relevant screening programs, the Ministry of Health has implemented Cumulative Preventive Care Bonuses. Through this program, eligible family doctors who practice as part of a Patient Enrolment Model, meaning, patients are formally rostered to a family doctor, may receive bonuses for maintaining specified levels of preventive care for their enrolled patients. Participant navigation: After a participant has an abnormal screening result, their Ontario Breast Screening Program (OBSP) site will notify their family doctor or nurse practitioner and may help to schedule a timely follow-up appointment. A participant with an abnormal mammogram who does not have a family doctor or nurse practitioner will be assigned a doctor who will follow them to diagnosis. If the participant does have breast cancer, they will be referred to a specialist for further care and management.QCProvider reminders and recall systemsMobile screening clinicsProviding transportation to screening servicesNBEducation (groups)Participant reminders and correspondenceMedia (social media, radio, transit ads) Provider correspondenceBilingual program materialsCommunity engagement for program feedbackLeverage learnings from under screened population projectPatient NavigationOffering virtual and in person education sessions on cancer screening programs in general, and specific to each screening site as requested by the public, health care providers, regional health authorities, community groups or special interest groups.Some health zones send letters to participants to remind of screening appointments or that it is time to re-book screening. Every screening site includes an additional information sheet about breast density with the screening result letters mailed to participants.Coordinated communication and awareness strategies are planned regularly throughout the year to promote and increase visibility of provincial cancer screening programs via various media such as radio ads, targeted digital ads, Facebook, Twitter, billboard and transit ads, website, animated and testimonial videos) Screening sites send result correspondence to primary care providers to alert them of screening results.ALL program correspondence, educational and promotional materials are offered in English and French. The program offers a toll-free phone line for public inquiries on cancer screening which is answered by bilingual staff.Public surveys have been offered by phone, online and following education sessions. Feedback provided to the program is collected and evaluated regularly.Plan to leverage the recommendations from the ongoing project ‘Developing Strategies for Underscreened Populations through Community Engagement’. Breast health navigation services are available to patients in most health zones across the province.NSMedia (mass)The coordinator for the mobile van places radio ads about upcoming mobile breast screening dates and locations.PEBusiness cards for physician office useEducational sessions with groups & new physician groupsMedia adsHealth fairsReminder letters for recallsPromotional itemsExtended hours of operation one day per week as well as Saturday appointmentsNLClient remindersProvider reminders and recall systemsPatient navigation
36. Strategies to Improve Breast Screening for First Nations, Inuit, and Métis (1/2)P/TIntended AudiencesStrategies used Strategy co-developed with community? Description of activities to improve screening for First Nations, Inuit, and MétisNTFirst NationsInuitMétisEducation Media (small and mass)Client reminder Recall systemPatient navigationHealthcare provider cultural competency trainingAll: ✓Breast Cancer Screening awareness kits were developed and distributed to the community health representatives in all community health centres to promote education at a local levelSocial media posts created and launched on the Northwest Territories Health and Social Services social media platforms (Twitter, Facebook, instgram) Reminder letters mailed to patientsRecall system for patients in place 1:1 health education available with HCP’s in primary care clinics and community health centresBCFirst NationsWebsitePrint resourcesPeer support materialsProvider materialsMobile screening First Nations communitiesCommunity-based outreachPatient videosAll: ✓BC Cancer is partnering with First Nations Health Authority to co-design interventions and promotional activities to engage First Nations population in BC. Breast screening services are also delivered to First Nations communities via the mobile mammography service.ABFirst NationsInuitMétisEducation (one on one and group)Client invitation and remindersMedia (small and mass)Provider assessment and feedbackMobile screening clinicsHealthcare provider cultural competency trainingDevelopment of culturally safe materials and resourcesDirect community engagement to co-design programs1. ✓2. 3. ✓4. 5. ✓6. ✓7. ✓8. ✓Partner with Indigenous representatives to conduct screening disparities evaluations and use findings to inform strategies to improve screening in Indigenous populations. Share evidence and learnings with service providers to provide culturally safe care. Work with Indigenous partners to develop and provide culturally appropriate information. SKFirst NationsMétisFirst Nations and Métis Cancer Surveillance strategyAll: ✓Outreach manager and program coordinators working with communities to identify needs and gaps in care.Adjusting mobile route to serve the communities when it works best for themEducating staff on cultural safety and competencyWorking with communications to develop culturally safe materials and resourcesMBFirst NationsMétisComprehensive letter campaignsInformative web siteInterpreter service availableAccessibility – 2 mobile clinics, 4 fixed locationsSocial media (Facebook) promoting mobile clinicsCulturally sensitive appointment booking processesProgram arranges and funds group flights for communities without road access to mammogram clinicsAll: ✓Community engagement and outreach through Prevention and Screening ProgramPartnerships with Regional Health Authorities, Nursing Stations, Health Directors, tribal councils, Wellness Centers, healthcare providers and valued stakeholdersPartnership with Community Engagement Liaisons.Mobile screening vehicles hosted on First Nation community.
37. Strategies to Improve Breast Screening for First Nations, Inuit, and Métis(2/2)JurisdictionIntended AudiencesStrategies used Strategy co-developed with community? Description of activities to improve screening for First Nations, Inuit, and MétisON*First NationsInuitMétisGroup educationMass mediaDevelopment of culturally safe materials and resources Provider reminders (Sioux Lookout area only)Mobile screening clinics (North West only)Providing transportation to screening services (for First Nations through Non-Insured Health Benefits [NIHN])Promotion of health literacyDirect community engagement to co-design programsAll: ✓Through the Indigenous Cancer Care Unit (ICCU), Regional Indigenous Cancer Leads and regional teams, communities are engaged to inform programs/initiatives to improve education and awareness of cancer screening. The ICCU is currently engaged in a study to investigate current correspondence and identify methods to enhance participant reminders. Ontario Health (Cancer Care Ontario) sends reminders following cancer screening invitation and recall letters to all eligible people in Ontario. A grant received by Dr. Jill Tinmouth and Dr. Amanda Shephard (“Catching Cancer Early how well do Ontario screening programs perform for First Nations and Métis persons?”) will provide Ontario Health (Cancer Care Ontario) with strategies to improve participation for First Nations and Métis people and may inform cancer screening recommendations in these populationsContinued ICCU support for the Cancer Screening Fact Sheets, Toolkit, and awareness postcards/posters which were designed and tailored with and for each First Nation, Inuit and Métis population. Cancer 101 Video: Ontario Health (Cancer Care Ontario) made this video for First Nations people. The video gives basic cancer information and answers many common questions about cancer. Other groups that helped make the video are CAREX Canada, the Occupational Cancer Research Centre and the Canadian Cancer Society. The Screening Activity Report (SAR) is an online report, which provides screening data to help family doctors improve their cancer screening rates and appropriate follow-up. The report allows family doctors to quickly find specific cancer screening information for each patient, including those who are overdue or have never been screened. In June 2018, the SAR was expanded to the Sioux Lookout Zone, which consists of several First Nations communities, providing non-patient enrollment model physicians and nurses access to their community data. This SAR was developed specifically for the Sioux Lookout municipality and the 27 First Nation communities that reside in the Sioux Lookout Zone. The ICCU continues to raise awareness with regional and community partners of medical transportation coverage available to eligible First Nations through the First Nations and Inuit Health Branch Non-Insured Health Benefits (NIHB) for breast cancer screening The ICCU and Northwestern Regional Cancer Program in partnership with communities jointly plan community events to provide access to screening through a mobile screening coach in the North West region. Through the relationships developed and fostered by the ICCU, regional teams have been able to continue working with communities as guided through the First Nations, Inuit, Métis and urban Indigenous Cancer StrategyQCFirst NationsInuitMétisMobile screening clinicsProviding transportation to screening services NBFirst NationsMétisGroup educationLeverage learnings from the project ‘Developing Strategies for Underscreened Populations through Community Engagement’ 1. ✓ (based on invitation to participate)2. The program offers group presentations upon request from First Nations Communities based on education needs for targeted audience. Plan to leverage the recommendations from the ongoing underscreening population project being conducted in NB.NS^First NationsPatient Navigator Patient navigator maintains community engagement with First Nations Health Directors.PEFirst NationsHealth fairsSocial media adsEducational clinics Promotional items Participation in educational sessions (individually) at health fairs as well as group educational presentations, reminder letters & recall lettersON: *Listed activities are not inclusive for all First Nations, Inuit and Métis populations. More information about the First Nations, Inuit, Métis and urban Indigenous Cancer Strategy can be found here: https://www.cancercareontario.ca/en/cancer-care-ontario/programs/aboriginal-programs/indigenous-cancer-strategyNS: ^Due to the COVID-19 pandemic, health fairs at First Nations communities that the Patient Navigator would have attended, were cancelled.
38. Strategies to Improve Screening for Underserved Populations (1/3)P/TIntended AudiencesStrategies used Strategy co-developed with community? Description of activities to improve screening for underserved populationsNTLow-IncomeImmigrants and refugeesRacial or ethnic minoritiesSpecific cultural groupsNon-English and Non-French SpeakersPeople without a primary care providerPeople with co-morbidities or chronic illnessPeople with physical disabilitiesPeople who are houselessPeople who live in rural and remote communitiesEducationMedia (small and mass)Opportunities for self-referralClient reminderRecall systemPatient navigationHelathcare provider cultural competency trainingAccess to interpreter services (site specific)All: ✓ Breast Cancer Screening awareness kits were developed and distributed to the community health representatives in all community health centres to promote education at a local levelSocial media posts created and launched on the Northwest Territories Health and Social Services social media platforms (Twitter, Facebook, instgram) Reminder letters mailed to patients1:1 health education available with HCP’s in primary care clinics and community health centresRe-design breast cancer screening posters, brochures and FAQ’s (including translation of materials to all 11 official languages of the NT). BCRacial or ethnic minoritiesNon-English and Non-French SpeakersPeople with physical disabilitiesTranslated and culturally safe materialsEngagement with community groupsTargeted media campaignsWebsitePrinted materials BC Cancer Breast Screening is inclusive by featuring and targeting under-served communities in its materials and as part of its outreach strategy.ABLow-IncomeImmigrants and refugeesRacial or ethnic minoritiesSpecific cultural groupsNon-English and Non-French SpeakersEducation (one on one and group)Client invitation and remindersMedia (small and mass)Provider assessment and feedbackHealthcare provider cultural competency trainingDevelopment of culturally safe materials and resourcesDirect community engagement to co-design programs✓ ✓ ✓✓✓Been engaged in a creating health equity project* for several years with data identified lower screening subpopulations in northeast Calgary to co-design strategies with the intent to scale and spread effective methods across Alberta. SKLow-IncomeImmigrants and refugeesRural and remote locationsPeople without a PCPNo PCP needed to attendMobile unit to avoid unnecessary costsEducation sessions with new to Canada populationsAll: ✓Coordinators provide education on breast screening at local community health centres, Open Door Society Community Fairs and also do classroom presentations both via Open Door Society and Sask Polytech (for new immigrants). Education sessions include pictorial presentations to help comprehension of contentMBNewcomersLow incomeSpecific cultural groupsPeople with mental illness or physical disabilitiesComprehensive letter campaignsInformative web siteInterpreter service availableAccessibility – 2 mobile clinics, 4 fixed locationsSocial media (Facebook) promoting mobile clinicsPCP booking request form for underscreened personsAll: ✓Cancer screening education module created with and for educators with students with low literacyCoordinating interpreter services with appointment timesTranslation document included in all public facing lettersScheduling longer appointments for those individuals who require longer appointment times for physical or emotional reasonsAB: *Current stage is funded by CPAC through the Developing Strategies for Underscreened Populations through Community Engagement grant.
39. Strategies to Improve Screening for Underserved Populations (2/3)P/TIntended AudiencesStrategies used Strategy co-developed with community? Description of activities to improve screening for underserved populationsONRacial or ethnic minoritiesSpecific cultural groupsNon-English and Non-French SpeakersLow-incomePeople without a primary care providerImmigrants and refugeesSpecific geographic areas (e.g., postal codes)People who missed their routine cancer screening test due to COVID-19Mass media Development of culturally safe materials and resourcesTranslation serviceMobile screening clinicsSelf-referral Reducing out of pocket costsChanges to correspondence eligibilityScreening awareness campaignOntario Health (Cancer Care Ontario) has a Breast Cancer Awareness Month (BCAM) campaign each October. The campaign includes the development and dissemination of promotional materials to regions. These materials include images which are representative of diverse groups.Ontario Health (Cancer Care Ontario) will translate program material and inquiry responses in various languages upon request.Ontario has two mobile screening coaches that offer cancer screening services (including breast screening) in the North West and Hamilton Niagara Haldimand Brant regions.A referral from a primary care provider is not required for screening through the Ontario Breast Screening Program (OBSP)_Screening through the OBSP is free for those eligible for the program. Ontario Health Insurance Plan coverage is also not required for people eligible for the OBSP. The Ontario Ministry of Health issued a directive to pause non-essential screening services in the spring of 2020 as a result of the COVID-19 pandemic. This included a pause in invitation and recall letters, which gradually resumed beginning in December 2020. Recognizing that people who were 74 during the correspondence pause may have since turned 75 (and would no longer be eligible to receive letters within our typical correspondence campaign), the upper age limit for invitation and recall letter correspondence campaigns was extended by one year to ensure those who did not screen due to the pandemic receive notifications to screenThe Ontario’s Ministry of Health will be leading a public campaign to remind people about the importance of regular cancer screening in September 2021 and have provided Ontario Health (Cancer Care Ontario) with support to develop additional strategies to support COVID-19 recoveryQCPeople without a primary care providerVoluntary Program PCP is assigned to the participant NBPeople without a primary care providerSpecific geographic areaImmigrants and refugeesProgram provides information on local breast screening clinics offering mammograms to those without a PCP Target strategies to improve participation.Provide program Information/education by working with Multicultural Associations.All: ✓Participants can call toll free screening line or go to the GNB website to access information on available clinics offering mammography to eligible participants.Using GIS mapping, the program is able to identify areas of low participation in order to further assess community needs and services. Offer informational sessions (virtual or in person) and/or promotional materials with screening information; assess information and language needs and adapt or develop tools, when able.NS^Incarcerated peopleNew immigrantsEducation (group)The Patient Navigator attends a Wellness clinic every year at a federal women’s prison, and provides breast screening information to the inmates. They also educate the medical staff on how to request mammography screening for the inmates.The Program Coordinator provides breast screening education to new immigrant individuals at the Immigrant Services Association of Nova Scotia (ISANS).NS: ^Due to the COVID-19 pandemic, some pre-planned presentations at the Immigrant Services Association of Nova Scotia (ISANS) were cancelled.
40. Strategies to Improve Screening for Underserved Populations (3/3)P/TIntended AudiencesStrategies used Strategy co-developed with community? Description of activities to improve screening for underserved populationsPE~Cultural groups Non-English speakers People without a PCPTranslated materials Translated materials Access to translation services Participants without PCP can access servicesUpdates pending for wheelchair access washroomLarger changerooms with equipment updatesNLLow-IncomeImmigrants and refugeesPeople with mental illnessPeople with physical disabilitiesPeople who are houseless Ongoing work with Regional Health Authorities collaborative clinics for people without access to primary care etc.PE: ~Utilize various translated materials to assist individuals with the mammography process
41. Strategies to Improve Access to Screening for Rural and Remote PopulationsP/TStrategies used Strategy co-developed with community? Description of activities to improve screening access for rural and remote populationsNTProviding transportation to screening servicesProvider reminders and recall systemsPatient navigationAccess to interpreter servicesAll: ✓Medical travel coordinated through the community health centres when mammography not offered locallyRecall systems in place at a local levelBCMobile mammography vehiclesMobile mammography vehicles provide service to rural and remote populations. BC Cancer Breast Screening promotes these stops through social and traditional media, and digital advertising.ABEducation (one on one and group)Client mobile announcement lettersMedia (small and mass)Provider assessment and feedbackMobile screening clinicsPatient navigation ✓✓Facilitated referral and provision of results to navigation program to ensure abnormal screens are followed up in timely manner.Timed correspondence to mobile schedule. Pilot nurse practitioner led integrated mobile screening services (mammogram, Pap, and FIT). SKMobile unit✓Invitations sent to invite participant to closest screening location.MBComprehensive letter campaignsInformative web siteAccessibility – 2 mobile clinics, 4 fixed locationsSocial media (Facebook) promoting mobile clinicsPCP booking request form for underscreened personsAll: ✓ONMobile screening clinics ✓Ontario has mobile screening coaches that offer cancer screening services including breast screening in the North West and Hamilton Niagara Haldimand Brant regions.QCMobile screening clinicsProviding transportation to screening servicesMobile screening clinics are transported by plane, train and boat to remote locations.NBDirect mailing of program invitation to eligible populationAwaiting results of Under-screened Population Project1. 2. ✓Program invitation letters are mailed directly to participant regardless of area of residence.Plan to incorporate recommendations from the project ‘Developing Strategies for Underscreened Populations through Community Engagement’.NSMedia (mass) The coordinator for the mobile van places radio ads about upcoming mobile breast screening dates and locations.PEExtended program hours Appointments available for evening & weekends NL Currently have a working group for the establishment of a satellite breast screening clinic in Happy-Valley Goose Bay (Labrador-Grenfell Health Region)
42. Strategies to Improve Screening for LGBTQ2S+ PeopleP/TStrategies used Strategy co-developed with community? Description of activities to improve screening access for rural and remote populationsBCTransgender peopleWebsitePrinted materialsProvider educationAll: ✓BC Cancer Breast Screening provides information and education about screening guidance for transgender persons.ABPeople identifying as LGBTQ2S+PCP of LGBTQ2S+ people Development of culturally safe materials and resourcesDirect community engagement to co-design programsAll: ✓In early stages of engagement with representatives from LGBTQ2S+ communities to develop resources, appropriate inclusive language in correspondence, and supports for PCPs. Exploring methods to modernize how sex/gender data collection can help inform appropriate screening engagement. SKLGBTQ2S+Partnerships ✓Partnership with OUT Saskatoon and Health Navigators to build more inclusive screening software.MBLGBTQ2S+Inclusive guidelines ✓Screening recommendations for trans people are published in our guidelinesInclusive language used in all materials and websiteBreastCheck staff have participated in culture safety training regarding LGBTQ2S+ populationsONNon-binary and gender diverse peopleOntario Health (Cancer Care Ontario) staffOverarching Policy for the Screening of Trans People in the Ontario Breast Screening Program and the Ontario Cervical Screening Program Educational webinars✓*✓** In March 2019, Ontario Health (Cancer Care Ontario) released the Overarching Policy for Screening of Trans People in the Ontario Breast Screening Program and Ontario Cervical Screening Program. The policy contains 17 recommendations on screening eligibility, interval and method for trans people at average and increased risk of breast and cervical cancer. The policy can be found at: www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/61546. A plan to implement the policy recommendations is currently being developed. Ontario Health (Cancer Care Ontario) is moving towards using gender-neutral language in screening products, wherever possible. Newly developed program resources in the Ontario Breast Screening Program will include gender-aneutral and inclusive language (e.g., referring to “people” as opposed to “women”); older materials are in the process of being updated.Ontario Health (Cancer Care Ontario) staff participated in webinars on better serving the LGBTQ2S+ community in healthcare and cancer screening (i.e., access, eligibility) NBGeneral publicInclusive language Reviewing and adapting program correspondence, materials and media for more inclusive language and images.NSTransgender peopleDeveloped draft transgender screening guidelines. NSBSP plans to conduct focus groups to learn more about how to make breast screening more accessible to the transgender population.PEExtended hours & evening appointments All gender washrooms *ON: Advocates, experts, and community members with expertise in better serving the LGBTQ2S+ community in healthcare (e.g., Rainbow Health Ontario) were involved in the development of the policy **ON: Delivered by Rainbow Health Ontario