

65 Clinical Geriatrics Program Attending Physician MSKCC Professor of Medicine Weill Cornell Medical College President International Society of Geriatric Oncology Disclosure No conflict of ID: 913974
Download Presentation The PPT/PDF document "Supportive Care Stuart M. Lichtman, MD" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.









Slide1
Supportive Care
Stuart M. Lichtman, MD65+ Clinical Geriatrics ProgramAttending Physician, MSKCCProfessor of Medicine, Weill Cornell Medical CollegePresident, International Society of Geriatric Oncology
Slide2Disclosure
No conflict of interests
Slide3SIOG
Thank you…for attendingfor your dedicationfor your enthusiasmYou are now part of a new familyYou are never alone
Slide4We’ve come a long way…
Slide5Where we’ve been
1980s: what’s geriatric oncology?1990s: sounds interesting; maybe we should review what is known-CALGB Cancer in the Elderly2000: SIOG begins2000s: lets start doing studies and study patient outcomes2007-CARG2010s: we are starting to learn about older cancer patients and how to treat them2018: we know a lot, but need to know more; we are great at predicting; we have to intervene and prove the benefit
Slide6SIOG Priorities
Viability of the organizationIncrease SIOG membership with emphasis on trainees; need to emphasize the value of membershipFundingIncorporate geriatric oncology principles into routine practiceRaise professional awareness of geriatric oncology and SIOG
Slide7Viability of the organization
Increasing membershipMaintain current membersBringing in new member particularly traineesWe need to ‘sell’ the idea that all adult oncologist are geriatric oncologists, i.e. need to know some aspect of basic geriatric principlesthis is particularly true to those feel that GO is irrelevant to their practiceDemographics should sell itselfProblem: too little time, too many organizations and memberships
Slide8SIOG Involvement
Need to expand the ‘big tent’ of SIOGIncrease involvement of other specialtiesNursingPT/OTGeriatric pharmacyRadiation oncologySurgical subspecialtiesRadiologists, i.e. interventionalistsNutritionNon traditional treatments, i.e. acupunctureYoung SIOG
Slide9Value of membership
Annual meetingJournalCMEE-learningGuidelinesParticipation in committees
Slide10Recent Guidelines
Management of prostate cancerRadiopharmaceuticalsAdherence to oral cancer therapyNutritionMelanomaPractical aspects of GAPlanning: renal cell, quality of life, corticosteroids, APL
Slide11Raise professional awareness of geriatric oncology and SIOG
ASCO, ESMO, EONS, ONS, etc etcHave to actively participate and be advocatesGrass roots efforts in home institutionsEncourage fellowsJournal reviews
Slide12Engagement in SIOG
MentorshipCommitteesTaskforcesYoung SIOGNAHSpeakersJournal ReviewersNot intimidating—inclusive
Slide13Incorporate geriatric oncology principles into routine practice
Why do I need to know Geriatric Oncology; I know how to take care of older patients…Show that developing predictive models add to or are better than clinical judgment, i.e. CARG and CRASH scoresPerformance status does not correlate with functional statusMuch of the assessment can be self administered or with help; role of technology; does not have to be time consuming or complicatedIncreasing data in medical oncology and surgery that some GA is useful
Slide142015
Slide15ASCO
Geriatric guidelinesMohile SG, Dale W, Somerfield MR, et al.: Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J Clin Oncol 2018Modernizing clinical trial eligibilityLichtman SM, Harvey RD, Smit M-AD, et al. Modernizing Clinical Trial Eligibility Criteria: Recommendations of the American Society of Clinical Oncology–Friends of Cancer Research Organ Dysfunction, Prior or Concurrent Malignancy, and Comorbidities Working Group. Journal of Clinical Oncology 2017Clinical trial design
Wildiers H, Mauer M, Pallis A, et al. End points and trial design in geriatric oncology research: a joint European
organisation
for research and treatment of cancer--Alliance for Clinical Trials in Oncology--International Society Of Geriatric Oncology position article. J Clin Oncol 2013
Slide16All adult oncologists are geriatric oncologists…
Slide17All adult oncologists are geriatric oncologists…
they just don’t know it yet
Slide18National Cancer Institute
Sponsored Trials
Essentially no data for patients 80+
Slide19Geriatric Oncology
Expanding older patient populationUnique needsRoutine evaluation is inadequateTruly personalized medicine
Some form of comprehensive geriatric assessment modified for oncology care
Predictive models of survival and functional decline exist (Soubeyran, 2012;
eprognosis
; G8)
Predictive models of toxicity (CARG and CRASH scores)
Clinical trials have not met the needs of older patients
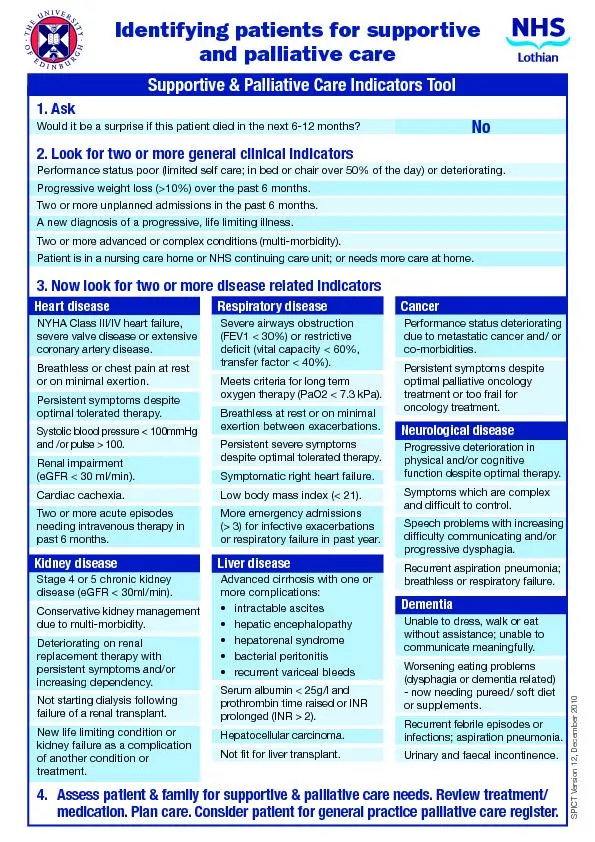
Slide20Palliative Care Definition
Palliative care End of life care
…particularly for older patients
Slide21WHO Definition of Palliative Care
Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.
Slide22WHO Definition
provides relief from pain and other distressing symptoms;affirms life and regards dying as a normal process;intends neither to hasten or postpone death;integrates the psychological and spiritual aspects of patient care;
offers a support system to help patients live as actively as possible until death;
offers a support system to help the family cope during the patients illness and in their own bereavement;
Slide23WHO Definition
uses a team approach to address the needs of patients and their families, including bereavement counseling, if indicated;will enhance quality of life, and may also positively influence the course of illness;is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications.
Slide24ASCO 2012: Integration of palliative care…
Palliative care as part of standard cancer care for all patients with metastatic disease and/or significant symptom burdenRecognizes that palliative care is a source of confusion and controversyWho should provide it?
Who it encompasses?
When and how it can help patients and their families?
Slide25Palliative Care in Older Patients
The best way to provide palliative/supportive care is to:Evaluate the patients in a geriatric specific manner including setting realistic goalsDose patients appropriately accounting for functional and physiologic status, i.e.
endorgan dysfunction
Provide appropriate supportive care
Antiemetics, pain, hydration, etc.
Understand patients desires and beliefs
Beneficial in older patients
Slide26Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer
2010
Slide27Temel, et al. Palliative Care
Slide28Temel, et al. Palliative Care
Half the patients were older than 65 years
Slide29Mean Change in Quality-of-Life Scores from Baseline to 12 Weeks in the Two Study Groups
Temel JS et al. N Engl J Med 2010;363:733-742
Early intervention improves all quality of life outcomes
Slide30Twelve-Week Outcomes of Assessments of Mood
Temel JS et al. N Engl J Med 2010;363:733-742
Slide31Kaplan–Meier Estimates of Survival According to Study Group
Temel JS et al. N Engl J Med 2010;363:733-742
Slide32Early Palliative Care: Improved Outcomes
Symptom managementPain, nausea, etc.Quality of life
Prognostic understandingCaregiver outcomes
Mood
End of life outcomes
Survival
Resource utilization
Slide33Quality of end of life care
Patients face many issues at the end of lifeCoping issuesComplications of dying
Practical issuesPhysical symptoms; fear of suffering
Family
Spouse
Children
MacKenzie, ASCO 2016
Slide34Evaluation
NutritionMini nutritional assessmentDoes the patient want to eat?Has there been significant weight loss
Cognition
Mini cog
Capacity to understand situation and make decisions
Delirium
Functional Status
ADL/IADL
Gait speed
Falls
Decline in IADL associated with greater frailty
ADL needs
Slide35Evaluation
Geriatric syndromes-increased risk of mortality and can worsen end of life symptomsSensory impairmentIncontinence
Falls/mobilityDepression
Delirium
Patient preferences and values
Discuss early and often; patient alone
“Based on your health...”
“Based on your values…”
Slide36Older Patients Symptom Burden
Palliative care may be considered to extend to survivorshipSurvivorship includes not just patients in remission but where cancer is a chronic diseaseChronic toxicity of therapy will require various forms of palliation
Particularly important in older patients
Slide37Palliative Care Key Points
Improves important outcomes for patients with cancer as been shown in five randomized controlled trialsASCO recommends early integration of palliative care into comprehensive cancer care for patients with advanced disease and/or significant symptom burdenOutcome improvements seen with early intervention
More research in specific circumstances, particularly older patients with their unique needs
Chronic toxicity
Survivorship issues
Clinical trials of survivorship and end of life need to performed in older patients similar to therapeutic trials
Slide38Vulnerable Populations
Quality of lifeAvoidance of toxicityAppropriate evaluationSurvivorship
Long term toxicities
Slide39Some of the issues to consider
Risk of febrile neutropeniaNausea and vomitingBone health
AnemiaDepression
Sleep Disorders
Fatigue
Pain
Slide40ASCO Guidelines-Universal Dataset?
Mohile, et al. JCO, 2018
Slide41Assessment tools
Maintenance of independence and function is criticalADL/IADLCGA (comprehensive geriatric assessment)
VES-13 (in NCCN guidelines)
G8
PS
Measures of comorbidity (Charlson, CIRS-G)
History and physical
Observation of patient; memory
Laboratory
Chemistries particularly renal function (calculate CrCl), anemia, albumin
Cardiovascular evaluation
Weight and BMI
Slide42Assessment Does Not Have to Be Complicated
Gait speed-ability to walk 1-2 blocksHistory of fallsWhere does the patient live?
Eliminate unnecessary medications-polypharmacyAsk about ADL/IADL
Social supports
Memory/cognition
Patients can do this while waiting
Slide43Avoidance of Toxicity
(1) impaired functional status - modification of cancer treatment regimen and evaluation of fall risk(2) in patients with impaired cognition assessing the presence of a caregiver and limiting the complexity of treatment.(3) in patients with poor social support assessing patient safety/tolerability and caregiver support(4) assessing the safety of treatment for patients with impaired physical performance and
(5) addressing supportive care and evaluating drug tolerance
for patients with poor nutritional status.
Slide44Avoidance of Toxicity
Appropriate dose and scheduleFunctional status, organ functionSocial supportsHematopoietic supportAntiemetic supportMay require more frequent visit to monitor labs, hydration status, etc.
Slide45Survivorship
Slide46Survivorship
Slide47Survivorship by Age
Slide48Survivorship by Age
46% of cancer survivors are 70 years and older
Slide49All oncologists are geriatric oncologists….
Survivorship Makes Us All GeriatriciansAging of the population
Risk of cancer increases with age
Specific needs of older patients
More complex options for treatment with toxicities
Markedly heterogeneous population
Comorbidity complicates toxicity of therapy and long term outcomes
Truly personalized medicine
Slide50Age at prevalence
Slide51Geriatric Knowledge Required
New York Times
Slide52Life Expectancy
Walter, et al. 2001
Slide53Survival
Incorporates:
-cancer vs. no cancer
-comorbidities
-dependence
Slide54Specific Toxicities
Slide55Long Term Toxicity into Survivorship
Shahrokni, Wu, Carter, Lichtman. Clin Geriatr Med, 2016
Slide56Long Term Toxicity into Survivorship
Shahrokni, Wu, Carter, Lichtman. Clin Geriatr Med, 2016
Slide57Chronic toxicity
Cognitive impairmentCardiotoxicityDepression and anxietyOtotoxicity
Imbalance and lack of coordination
Osteoporosis
Metabolic syndrome
Second malignancy
Sexual and vaginal dysfunction
Shahrokni A, Wu AJ, Carter J, Lichtman SM: Long-term Toxicity of Cancer Treatment in Older Patients. Clin Geriatr Med 32:63-80, 2016
Slide58Cognitive Impairment
Unrecognized, pre-existing problems may exacerbate, i.e. dementiaOften important to evaluate for depressionEliminate unnecessary medication: Beer’s list
HypnosedativesNarcotics
Anticholinergic drugs
May need formal evaluation, i.e. neuropsychologic testing
Hormonal evaluation particularly in immunotherapy era (checkpoint inhibitors, etc.)
Slide59Cardiotoxicity
Slide60Cardiotoxicity
Increased number of cardiotoxic drugs associated with prolonged survival requiring followup:Doxorubicin and other anthracyclinesLiposomal doxorubicin
Trastuzumab (Herceptin) and associated compounds
Control of hypertension
Increased use of anti-VEGF drugs,
i.e
bevacizumab (Avastin); trastuzumab emtansine (Kadcyla)
Control of diabetes
Pericardial and myocardial disorders in patients receiving prior thoracic irradiation
Volume status
QT interval-arrhythmias, electrophysiology
Slide61Balance and coordination
Chemotherapy induced peripheral neuropathy from taxanes, vinca alkaloidsLack of balance and coordination can lead to falls and subsequent injuriesFalls affect overall survival
Older patients more susceptible to toxicityComorbidities such as preexisting neuropathy, diabetes increase risk
Lichtman SM, Hurria A, Cirrincione CT, et al. Paclitaxel efficacy and toxicity in older women with metastatic breast cancer: combined analysis of CALGB 9342 and 9840. Ann Oncol 23:632-8, 2012
Slide62Balance and coordination
Recognize issueConsequences of peripheral neuropathyGait disturbancesRisk of falls
Driving; climbing stairsOccupational therapy helpful particularly to help hand function, i.e. dressing, opening jars, etc.
Physical therapy for fall prevention, increase lower extremity strength
Exercise programs
Drugs for symptom management are minimally effective and have toxicity, i.e. gabapentin
Slide63Muscle and bone health
Higher risk of osteoporosis and fracturesRisk factors:Therapy induced menopauseUse of aromatase inhibitors
Androgen deprivation therapy
Bone density evaluation
Treatment
Calcium and vitamin D supplementation
Exercise, sunlight
Bisphosphonates (zolendronic acid-Reclast)
Rank ligand inhibitors (denosumab-Prolia)
Slide64Fatigue
One of the most common long-term side effects of cancer therapy is fatigue. Exacerbated by comorbidity, i.e. heart and lung disease, anemia renal dysfunctionSymptom of fatigue that patients with cancer experience is different; not often alleviated by sleep and rest.
Patients who have undergone cancer treatment get fatigued after less activity than those who have not had cancer. The cause of this symptom is multifactorial:
Long term effects of therapy (eg, chemotherapy, radiation, biologic therapy, surgery), anemia, nutrition, anxiety and depression, sleep disorders, and drugs.
Slide65Fatigue-Polypharmacy can contribute
Polypharmacy, which is common in the elderly, can contribute. Specific drugs, such as anxiolytics, sleeping medicine, narcotics, and drugs that treat neuropathy (eg, gabapentin, pregabalin)Difficult issue; consider nonpharmacologic interventions such as exercise programs, psychological support in event of depression/anxiety
Avoid pharmacologic therapy
Amphetamines, modafinil
Corticosteroids
Cancer chemotherapy premedication
Symptom may be prolonged into survivorship, months to years
Slide66Long term effect of radiation therapy in elderly
Chronic fibrosis and its sequelae, i.e. obstructive uropathyEffect on CNS; may exacerbate cognitive impairmentXerostomia from head and neck therapy; impair nutrition; dental issues (not covered by Medicare)
Pulmonary fibrosisHeart disease, coronary disease, pericardial disease
Chronic GI effects, ie. Diarrhea, incontinence
Insufficiency fractures; painful, should not be confused with metastases, DJD, osteoporosis
Sexual dysfunction, i.e. vaginal dryness and stenosis; discomfort and inability to be appropriately examined
Secondary malignancy
Slide67Secondary malignancy as chronic toxicity
Older cancer survivors have approximately 15-20% incidence of a second cancerAML/MDS from chemotherapyTopoisomerase II inhibitors-less than 5 yearsAlkylators-greater than 5 years
Breast cancer from thoracic radiationIssue of genetic predisposition, i.e. BRCA, Lynch syndrome
Pelvic radiation
Radiation therapy for prostate cancer increase risk of cancer of the bladder, colon and rectum but absolute incidence is low
No increase risk in patients treated for rectal or endometrial cancer (Wiltnick, et al. JCO 2014)
Increase risk of external beam RT for endometrial cancer in patients less than 60 years (Onstrud, et al. JCO 2013)
Continue standard screening recommendations
Slide68Second Malignancy
Slide69Conclusion
Elderly patients are the majority of cancer survivors and their numbers are increasingComorbidity and the problems of aging combined with the effects of therapy will pose a challenging problem for clinicians and the health care systemSome form of geriatric assessment will be required to adequately evaluate the patients
Controlling comorbidity will be critical
Preventive health measures will be of critical importance
All clinicians will need to become geriatricians and/or geriatric oncologists
Slide70Thank you very much
lichtmas@mskcc.org
Slide71Slide72Thank you