
A Shared Responsibility Presenters Marty Crapper Executive Director Cheryl English Director of Programs and Services Brandice Hartin Manager of Primary Care Relationships with Commercial Interests none ID: 557635
Download Presentation The PPT/PDF document "Physician Retirement & Patient Exper..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.





Slide1
Physician Retirement & Patient Experience:A Shared ResponsibilitySlide2
PresentersMarty Crapper: Executive DirectorCheryl English: Director of Programs and Services Brandice Hartin: Manager of Primary CareRelationships with Commercial Interests: none
Grants/Research Support: none
Speakers Bureau/Honoraria: noneConsulting Fees: We wish! noneOther: noneSlide3
Mr. and Mrs. CrapperSlide4
Clients of a bank in Brighton for 40 yearsLongstanding relationship based on trustPersonal relationship with managerSlide5
Ways in which the bank offered helpWe notified patients with a prominent ad in the newspaper 3 months before we closedWe could not possibly contact each of our clients directlyYou will need to seek a new bank who will accept you on your own. Here is a list of bank manager namesGood luck!Slide6
Our Goal Today:
Share the experiences of managing the transition of
care for
patients in
Rideau Lakes Township and the village of Westport over
the past 10 years
Reflect on
three provider retirement “types” and
the variables that might result in higher patient satisfaction
Recommend approaches for funders, physicians and patients that could be used when we are faced with physician retirements in the future
Objectives
Given the certainty that every provider will eventually retire and that
every patient will experience provider transition
……..Slide7
Where is North Leeds?Slide8
Physician Retirements in North Leeds 2006-2015
700
1200
850
500
650
1000
750
5650 patients change doctors!Slide9Slide10Slide11
In 3 of the 5 physician retirements, there was little or no advanced planning for patients to ensure a smooth transition to a new provider.
How do
we
move towards
a health
system that guarantees patients a smooth transition when their provider retires?
KEY
ISSUESlide12
5 MD RETIREMENTS RESULTED IN TOTAL SHIFT OF 3,000 PEOPLE
IN NORTH LEEDS IN PAST
3-5 YEARS
3 of 5 had no advanced planning Slide13
Impacts Anxiety
Continuity of care
Provider Client therapeutic relationship *Trust breakdown
Provider burdensConfusion
Misinformation
*American Medical Association, 2003Slide14
Limited literature on effect of health outcomes & continuity of care when a provider leaves, however………
“
Comfort with a provider and trust were the attributes of the therapeutic relationship that are most poignantly mentioned by patients” Journal of General Internal Medicine, 2008Slide15
Capacity & SupportsTeam Based Retirement Administrative capacity
Support for clients ongoing
AbsorbedCoverage model in place Inter-professional team Communication capacity
Solo Provider Retirement Limited capacityLimited coverage
Communication barriers
Limited inter-professional support Slide16
Our Experiences Team based practice (internal CHC)
Solo Practice setting (less common in 2016 but still out there!)
LHIN funded pilot Slide17
Client Experience Slide18
What did we want to know?
Were there any differences in experiences for people who
had providers from different models?
What type of supports best help people who experience a loss of provider? Slide19
What We AskedAge (age 70 average)
Specific experience
(how they learned of their doctor leaving)
Emotional impact
What support did you receive?
What additional support would have helped you?Slide20
How We Asked Random telephone survey 20 from each of the 3 types: solo (unsupported), team (CHC) and LHIN funded pilot.
Name of previous doctor (for “type” assignment)
3 questions about overall satisfaction with the way they learned about and were supported through the transition to
a new provider.Slide21
How did you find out your doctor was leaving? Doctor told me directlyI received a letter
I received a phone call
I read it in the newspaperI heard it informally through a friend or neighbour
Other Slide22
How did you feel when you first foundout that your doctor was leaving?(Scale 0 to 5)
Confused vs. Not Confused
Anxious vs. CalmAlone vs. SupportedAngry vs. Not Angry
Other FeelingsSlide23
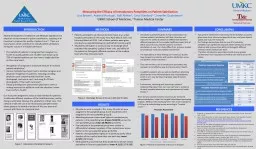
What types of support did you receive when you found out that your doctor was leaving?I received direct assistance from my doctor’s officeI was given the name and number of my new doctorI was provided enough medication for the length of time neededI got a call from someone at the new provider office quicklyOtherSlide24
Given your experience this past year,what do you think should happen when a doctor leaves or retires to make it a better process for the patient?Slide25Slide26
How did you find out that your doctor was leaving or retiring?Slide27
How did you feel when you first found out that your doctor was leaving or retiring?Slide28
What type of support or help did you receive when you got the news that your doctor was leaving or retiring?
Number of RespondentsSlide29
What
support
did you receive when you got the news that your doctor was
leaving?.....Other
The “free text” comments from clients of the solo providers who were informed by newspaper, word of mouth or letter are eye opening…..
I feel I got no help at all
I just had to search by myself
I got very little support.
There
was nothing in
place
I did not really get any assistance until the new service contacted me
Was
totally up to me
I had to do the leg work myself
I had to buy my files back and shop for a doctor
75% of the patients surveyed who had solo providers gave a negative answer to the question of type of support provided to them.I did not think this could happen in CanadaAbandoned, loss of trust, loss of sleep, felt like I was not importantSlide30
Team Supported Transition
I was given quite a bit of advance notice so I was able to prepare
I was fine
I did still access nursing support while I waited
It was ok as I was told not to worry and that a new doctor would be assigned.
I am happy with the new doctor
I was anxious about seeing a female doctorSlide31
What We Heard….There should be a plan & provider responsibility that results in immediate accessIt should not be up to me to find another MDPlanned assistance and direct help for patients
Much better communication when providers retire Slide32
What We Heard cont’d….The government should not let physicians decide on their own that they will not see a complex patient, there should be a processSomeone needs to be in charge of making sure patients get service The MD on their own did not have the resource to figure out the solution, support from the system is needed! Slide33
Transition PilotSlide34
Evolution Of Our Client Transition Pilot
How do we deal with influx of 1300 clients? Slide35
Pilot StructureFunded for 8 months, LHIN supported and in-kind contribution provided by CRCHC. Goal is to effectively transition clients to the existing CHC team.
Transition Team
Transitions Coordinator
Intake ReceptionistNurse Practitioner
Pharmacist
Existing Inter-professional team, SW, RD, RT, MD, NP, RN
1300 potential clients Slide36
Registration and TriageClients registered in person or online, forms at pharmacy or Dr. X’s office
Consent for release of information was signed by all new clients for release of records
Introductory letter outlining process and reassurance
Clients triaged and assigned a provider based on urgency, complexity of the individual, provider preferences, and scope of practiceSlide37
Triage ProcessSlide38
Case ExamplesSlide39
Content of Intake InterviewsIntroduction to the CHC
Health Questionnaire
EHR Entry and Chart ReviewSlide40
Barriers to TransitionTime and number of clients needing serviceCommunicationAccess for existing clientsNeeds of new clientsLack of trust from new clientsSlide41
TimelinesHow did we deal with lack of time?
~600 clients need to be seen from Apr to Nov
Six 30 min. intake assessments per day starting in April by the Transition Coordinator
How did we schedule appointments?Clients called in order of urgency and complexity for each assigned provider
Intake assessments completed prior to the Meet and Greet with the provider
Need for Meet and Greet appointment was determined during the intake assessmentSlide42
Case Example
What was my role with this client?Slide43
CommunicationSlide44
AccessHow did we address the need for our existing clients to be unaffected by the influx?Locum NP to accommodate the urgent needs and follow up appointments for existing clients
Existing clients managed as much as possible by members of our interdisciplinary team in order to free up the providers
Mental Health clients to social work Diabetes clients to DB programRequests for medication renewals to pharmacistSlide45
Needs of New ClientsHow did we address the urgent needs of the new
clients?
New clients were seen for urgent issues by primary care team even prior to
the intake assessmentNew clients were referred internally to members of our team
during
intake
Mental Health clients to social work
Clients on >5 medications to
Pharmacist
Diabetes
clients to DB programSlide46
Case ExampleClient D- 40 y.o man with Asperger’s who identified during the intake appointment that he felt depressed, stressed, anxious, ashamed, trapped, angry, and was suffering from suicidal ideationNever been seen by psychiatry
No counselling services provided
No psychiatric medicationsNo form of support other than his mother
How did we support this client?Slide47
TrustHow did we address the lack of trust?
By addressing the issues as the client brought them up
By identifying what is important to the client
What is important to you?
What are you worried about right now?
Why is it important to ask these questions
?Slide48
Case ExampleClient E- 50
y.o
female with hypertension, bipolar disorder, and fibromyalgia.
Biggest concern?
Teeth!
She reported constant taste of blood in her mouth, and teeth breaking off anytime she tries to eat something solid.Slide49
Lessons Learned
What worked Upfront intake admin support
Transitions Coordinator role was critical for triage & support Documentation & health record “work up”
Collaborative work with solo MD & staff
Social media messaging
Board of Directors role in communication
Improvements
Communication, communication, communication– INSIDE & OUT
R
educe steps for intake & registration process
Slide50
Transition Pilot Client Experience Slide51
How did you find out that your doctor was leaving or retiring?
0 20 40
60 80
% of respondentsSlide52
How did you feel when you first found out that your doctor was leaving or retiring?
_______________________________________________________
Most Negative Least Negative
0 1 2 3 4 5
Average Response to Scaling Questions Slide53
What type of support or help did you receive when you got the news that your doctor was leaving or retiring?
Number of RespondentsSlide54
Transition Pilot
What
type of support
did
you receive when you got the news that your doctor was
leaving?
I just had to wait for someone to call. A young lady
got in touch. She worked for the new doctors
office
I was introduced to a
pharmacist who helped me prepare for my visit with a new doctor.
W
as
told of new provider and given a f0rm to fill out
I had a phone call from the new service and they made an appointmentVery poor support, too little, too lateT
ook a long time to get appointmentI felt abandoned but fortunate that Country Roads stepped inSlide55
6 Months Later….I think that the idea of reaching out to patients on FB is a smart ideaI think your communication with the community is a big strengthYou helped me when my doctor retired, she did not give me much notice and I needed help, you were there for usProfessional and very efficient, the clinic runs like a charm
I think the new system of using a variety of professions is much more efficient than having one everyone see the doctor.Slide56
How do we move towards a health system that guarantees patients a smooth transition when their provider retires?
KEY
ISSUESlide57
Dr. Ian Shiozaki
Location:
Newboro
,
Ontario
History: Over 30 years in same location
Clients: 1200
Age 63
Team composition: 1 RN, 1 Medical Receptionist
Retirement Plans???Slide58
SHARED RESPONSIBILITY??