
AFO In Physical Rehabilitation Of children with Neglected Club foot ICRC Protocol A case study By Abdulmunaf Faruk PT Sulaiman Isah PO Outline Case study ICRC Approach Introduction ID: 1033521
Download Presentation The PPT/PDF document "Role of Ankle Foot Orthosis" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




1. Role of Ankle Foot Orthosis (AFO) In Physical Rehabilitation Of children with Neglected Club foot; ICRC ProtocolA case studyByAbdulmunaf Faruk (PT)Sulaiman Isah (PO)
2. OutlineCase studyICRC ApproachIntroductionCauseRisk FactorsPresentationComplication ManagementPonseti Method
3. Case StudyName: XYAge: 9 yearsGender: Male Occupation: A PupilAddress: Dorayi, KanoPresented on: 29th july, 2020
4. Case StudyA case of 8 year old boy presented to ICRC Dala Centre with TEV (Club foot)The deformity was 1st detected 20 days after birth, they went to MMSH kano, were the baby had serial casting with POP on a regular interval for six month. Still the deformity was not corrected, they were referred to this Hospital, the baby was 1st attended in A&E, they were prescribed TEV corrective shoes.
5. After one year, they stop using the shoes because it was too small for the child. When they present to hospital again after a year, the deformity still persist.They were then ask to come for another serial casting, for which the absconded for five years before they return to hospital, and were then advice for surgery which they couldn’t afford.
6. They presented to ICRC NOH-Dala centre on 29th july, 2020, when the boy was 8 years old.Refer to video one
7. ICRC Physical Rehabilitation model The ICRC PRP involves a multidisciplinary approach to rehabilitation Assessment Designing GoalImplementationCastingFabricationModificationTraining and Follow up
8. ICRC used a polyprophylene (PP) technologyIt is a special thermoplasticCan be mold to any shape of choiceCome in different coloursWe use the brown type for Arica
9. After assessment, it was found that the soft tissue yielded to stretching and the ankle joint is still mobile passively.Had initial casting for AFOThe cast was modifiedThen AFO was fabricatedThe child was fitted and started trainingRefer to video 2
10.
11. The child was followed every two weeks for six weeks.Then every month for four month, the boy was discharged and back to school.ICRC supported and follow up the boy’s management.Refer to video 3
12. Before After
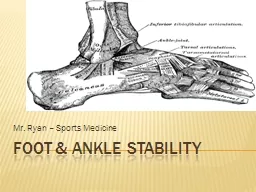
13. Club FootClubfoot is a congenital condition (present at birth) that causes a baby’s foot to turn inward or downward. It can be mild or severe and occur in one or both feet. In babies who have clubfoot, the tendons that connect their leg muscles to their heel are too short. These tight tendons cause the foot to twist out of shape.
14. Clubfoot is one of the most common congenital birth defects. It occurs in about 1 in every 1,000 babies born in the U.S. and affects more boys than girls. In fact, boys are twice as likely to be born with clubfoot.
15. CauseThe cause of clubfoot is unknown (idiopathic), but it may be a combination of genetics and environmental factors.
16. Risk FactorsFamily history. If either of the parents or their other children have had clubfoot, the baby is more likely to have it as well.Congenital conditions. In some cases, clubfoot can be associated with other abnormalities of the skeleton that are present at birth (congenital), such as spina bifida.
17. Environment. Smoking during pregnancy can significantly increase the baby's risk of clubfoot.Not enough amniotic fluid during pregnancy may increase the risk of clubfoot.
18. PresentationThe top of the foot is usually twisted downward and inward, increasing the arch and turning the heel inward.The foot may be turned so severely that it actually looks as if it's upside down.The affected leg or foot may be slightly shorter.The calf muscles in the affected leg are usually underdeveloped.
19.
20. ComplicationMovement. The affected foot may be slightly less flexible.Leg length. The affected leg may be slightly shorter, but generally does not cause significant problems with mobility.Shoe size. The affected foot may be up to 1 1/2 shoe sizes smaller than the unaffected foot.Calf size. The muscles of the calf on the affected side may always be wasted and smaller than those on the other side.Arthritis. Your child is likely to develop arthritis.
21. Poor self-image. The unusual appearance of the foot may make the child's body image a concern during the teen years.Inability to walk normally. The twist of the ankle may not allow the child to walk on the sole of the foot. To compensate, he or she may walk on the ball of the foot, the outside of the foot or even the top of the foot in severe cases.Abnormal gait, Problems stemming from walking adjustments.
22. PreventionThe cause of club foot is not known, therefore you can't completely prevent it. However, during pregnancy, you can limit baby's risk of birth defects, by:Avoiding smoking or spending time in smoky environmentsAvoid taking alcoholAvoiding drugs not approved or prescribed by the appropriate healthcare provider.Regular Ante-natal care
23. Managementclubfoot is not a painful condition,It can be corrected while a child is a still a baby. Treatment should begin a week or two after birth. Correction methods vary from manual foot manipulation over time to surgically fixing the foot.In rare cases, clubfoot is not completely correctable. With Ponseti reporting over 89% success rate.
24. The Ponseti methodThis involves combination of stretching and the used of a cast. The baby’s foot is stretched toward the correct position and then place in a cast on it to hold it there. Every week or so, the cast is removed, stretch the foot further toward the correct position, and re-cast. This will continue until the foot is fully in the correct position (usually several months).
25. Once the final cast is off, your baby will probably need to wear an abduction brace for a certain period. It could take several months or even a few years depending on initial presentation and follow up. When clubfoot is severe, surgery is often the best option.
26.
27.
28.