
Psychiatric Rehabilitation 18Month Longitudinal Study KeeHong Choi 12 L Felice Reddy 1 Nancy Liu 1 amp William D Spaulding 1 University of NebraskaLincoln 1 ID: 1042975
Download Presentation The PPT/PDF document "Introduction History of Childhood Abuse ..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


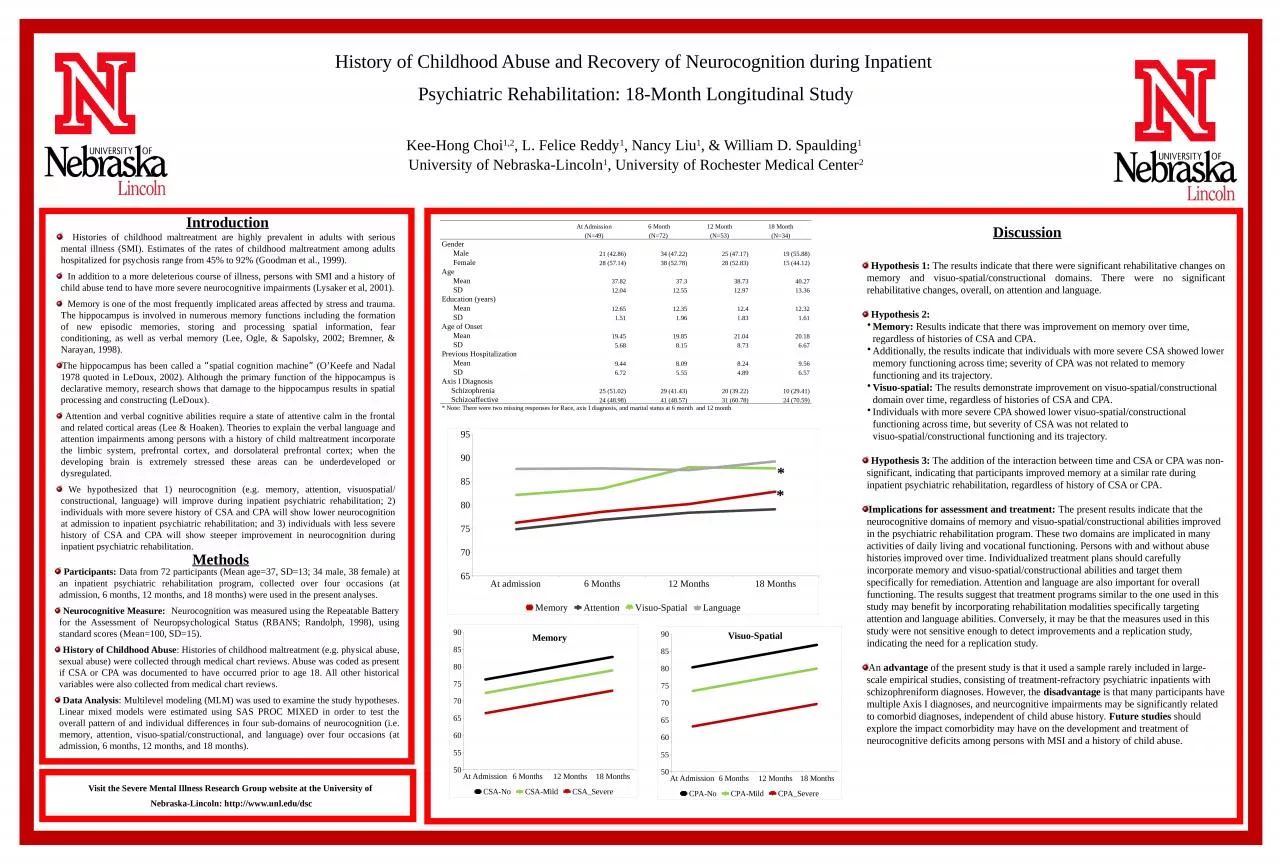
1. IntroductionHistory of Childhood Abuse and Recovery of Neurocognition during Inpatient Psychiatric Rehabilitation: 18-Month Longitudinal StudyKee-Hong Choi1,2, L. Felice Reddy1, Nancy Liu1, & William D. Spaulding1 University of Nebraska-Lincoln1, University of Rochester Medical Center2 Histories of childhood maltreatment are highly prevalent in adults with serious mental illness (SMI). Estimates of the rates of childhood maltreatment among adults hospitalized for psychosis range from 45% to 92% (Goodman et al., 1999). In addition to a more deleterious course of illness, persons with SMI and a history of child abuse tend to have more severe neurocognitive impairments (Lysaker et al, 2001). Memory is one of the most frequently implicated areas affected by stress and trauma. The hippocampus is involved in numerous memory functions including the formation of new episodic memories, storing and processing spatial information, fear conditioning, as well as verbal memory (Lee, Ogle, & Sapolsky, 2002; Bremner, & Narayan, 1998).The hippocampus has been called a “spatial cognition machine” (O’Keefe and Nadal 1978 quoted in LeDoux, 2002). Although the primary function of the hippocampus is declarative memory, research shows that damage to the hippocampus results in spatial processing and constructing (LeDoux). Attention and verbal cognitive abilities require a state of attentive calm in the frontal and related cortical areas (Lee & Hoaken). Theories to explain the verbal language and attention impairments among persons with a history of child maltreatment incorporate the limbic system, prefrontal cortex, and dorsolateral prefrontal cortex; when the developing brain is extremely stressed these areas can be underdeveloped or dysregulated. We hypothesized that 1) neurocognition (e.g. memory, attention, visuospatial/ constructional, language) will improve during inpatient psychiatric rehabilitation; 2) individuals with more severe history of CSA and CPA will show lower neurocognition at admission to inpatient psychiatric rehabilitation; and 3) individuals with less severe history of CSA and CPA will show steeper improvement in neurocognition during inpatient psychiatric rehabilitation.Methods Participants: Data from 72 participants (Mean age=37, SD=13; 34 male, 38 female) at an inpatient psychiatric rehabilitation program, collected over four occasions (at admission, 6 months, 12 months, and 18 months) were used in the present analyses. Neurocognitive Measure:: Neurocognition was measured using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS; Randolph, 1998), using standard scores (Mean=100, SD=15). History of Childhood Abuse: Histories of childhood maltreatment (e.g. physical abuse, sexual abuse) were collected through medical chart reviews. Abuse was coded as present if CSA or CPA was documented to have occurred prior to age 18. All other historical variables were also collected from medical chart reviews. Data Analysis: Multilevel modeling (MLM) was used to examine the study hypotheses. Linear mixed models were estimated using SAS PROC MIXED in order to test the overall pattern of and individual differences in four sub-domains of neurocognition (i.e. memory, attention, visuo-spatial/constructional, and language) over four occasions (at admission, 6 months, 12 months, and 18 months). Discussion Hypothesis 1: The results indicate that there were significant rehabilitative changes on memory and visuo-spatial/constructional domains. There were no significant rehabilitative changes, overall, on attention and language. Hypothesis 2: Memory: Results indicate that there was improvement on memory over time, regardless of histories of CSA and CPA. Additionally, the results indicate that individuals with more severe CSA showed lower memory functioning across time; severity of CPA was not related to memory functioning and its trajectory.Visuo-spatial: The results demonstrate improvement on visuo-spatial/constructional domain over time, regardless of histories of CSA and CPA. Individuals with more severe CPA showed lower visuo-spatial/constructional functioning across time, but severity of CSA was not related to visuo-spatial/constructional functioning and its trajectory. Hypothesis 3: The addition of the interaction between time and CSA or CPA was non-significant, indicating that participants improved memory at a similar rate during inpatient psychiatric rehabilitation, regardless of history of CSA or CPA.Implications for assessment and treatment: The present results indicate that the neurocognitive domains of memory and visuo-spatial/constructional abilities improved in the psychiatric rehabilitation program. These two domains are implicated in many activities of daily living and vocational functioning. Persons with and without abuse histories improved over time. Individualized treatment plans should carefully incorporate memory and visuo-spatial/constructional abilities and target them specifically for remediation. Attention and language are also important for overall functioning. The results suggest that treatment programs similar to the one used in this study may benefit by incorporating rehabilitation modalities specifically targeting attention and language abilities. Conversely, it may be that the measures used in this study were not sensitive enough to detect improvements and a replication study, indicating the need for a replication study. An advantage of the present study is that it used a sample rarely included in large-scale empirical studies, consisting of treatment-refractory psychiatric inpatients with schizophreniform diagnoses. However, the disadvantage is that many participants have multiple Axis I diagnoses, and neurcognitive impairments may be significantly related to comorbid diagnoses, independent of child abuse history. Future studies should explore the impact comorbidity may have on the development and treatment of neurocognitive deficits among persons with MSI and a history of child abuse. Visit the Severe Mental Illness Research Group website at the University of Nebraska-Lincoln: http://www.unl.edu/dsc At Admission 6 Month12 Month18 Month (N=49)(N=72)(N=53)(N=34)Gender Male21 (42.86)34 (47.22)25 (47.17)19 (55.88) Female28 (57.14)38 (52.78)28 (52.83)15 (44.12)Age Mean37.8237.338.7340.27 SD12.0412.5512.9713.36Education (years) Mean12.6512.3512.412.32 SD1.511.961.831.61Age of Onset Mean19.4519.8521.0420.18 SD5.688.158.736.67Previous Hospitalization Mean9.448.098.249.56 SD6.725.554.896.57Axis I Diagnosis Schizophrenia25 (51.02)29 (41.43)20 (39.22)10 (29.41) Schizoaffective24 (48.98)41 (48.57)31 (60.78)24 (70.59)* Note: There were two missing responses for Race, axis I diagnosis, and marital status at 6 month and 12 month**MemoryVisuo-Spatial
2.