
Presented by Dr Iram Naseer Moderated by Prof Iqbal Aziz BREAST CARCINOMA Breast cancer is most common malignancy in female Second to lung cancer Now the mortality rate ID: 920916
Download Presentation The PPT/PDF document "Management of breast cARCINOMA" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
Management of breast cARCINOMA
Presented by:Dr. Iram NaseerModerated by:Prof .Iqbal Aziz
Slide2BREAST CARCINOMA
•Breast cancer is most commonmalignancy in female •Second to lung cancer•Now the mortality rate is↓owing to early detection
•
Etiology of the vast majorityof breast cancer is unknown
Slide3RISK FACTORSAge
smokingpoor dietPersonal history of breast disFamily historyGenetic predispositionRadiation exposureExcess weight
Slide4Early menarcheLate menopause
Older age pregnancyRaceHormone therapyBirth control pillsLack of exerciseNullipara
Not breast feeding
AlcoholPrecancerous breast
changes
(
atypical
hyperplasia)
Slide5Slide6Diagnosis of breast cancer
History • breast mass • breast pain • nipple discharge • nipple or skin retraction • axillary mass or pain • arm swelling • symptoms of possible metastatic spread
Slide7Past medical history of breast disease
Family history of breast andother cancers with emphasis on gynaecological cancersReproductive history• age at menarche • age at first delivery • number of pregnancies, children and miscarriages • age at onset of menopause
• history of hormonal
viz OCP
Slide8Breast self exam
Slide9Slide10Physical examination
Breast mass – size – location (specified by clock position and distance from the edge of the areola) – shape – consistency – fixation to skin, pectoral muscle and chest wall –
multiplicity
Slide11Slide12Skin changes
– erythema (location and extent) – oedema (location and extent) – dimpling – infiltration– ulceration
Slide13nipple changes
– retraction – erythema – erosion and ulceration – discharge (specify)nodal status – axillary
nodes on both sides (number, size, location and fixation to other nodes or underlying structures
) – supraclavicular
nodes
Slide14Slide15RADIOLOGICAL INVESTIGATIONS
Mammography Nuclear Imaging(scintimammography) Ultrasonography Doppler Flow Studies Thermography Magnetic resonance imaging PET Scan
Slide16Mammography
Mammography is a special type of x raycan demonstrate microcalcifications smaller than 100 μmReveals a lesion , 1-2 years before it is palpablesupportive to biopsy
Slide17Slide18Types of mammography :
screening Diagnosticdone in asymptomatic women Diagnostic mammography is performed in symptomatic women
Slide19FINDINGS IN MAMMOGRAPHY
MASSESSpace occupying lesion Round or oval- benign Irregular - malignant CALCIFICATIONS <0.5mmheterogenous
mass
microcalcificatn
Slide20Mammogram – Difficult Case
•Heterogeneously dense breast •Cancer can be difficult to detect with this type of breast tissue •The fibroglandular tissue (white areas) may hide the tumor •The breasts of younger women contain more glands and ligaments resulting in dense breast tissue
Slide21Mammogram – Easier Case
With age, breast tissue becomes fattier and has fewer glands Cancer is relatively easy to detect in this type of breast tissue
Slide22Slide23Ultrasound screening
supplement to mammography use in routine screening of general populationrole in young patients and high risk patients
Slide24•As a screening device, fail to detect microcalcifications
•performed primarily to differentiate cystic from solid lesions •Ultrasonography is also useful for guiding the aspiration of cysts to provide cytologic specimens in FNAC
Slide25Magnetic Resonance Imaging
Modality for detecting breast cancer in women at high risk and in younger women. Detection of occult breast carcinoma in a patient
Slide26Evaluation of multifocal or bilateral tumor •Evaluation of invasive CA•Evaluation of suspected, extensive, high-grade carcinoma
•Monitoring of the response to neoadjuvant chemotherapy •Detection of recurrent breast cancer• Best modality for the breasts of women with implants
Slide27Contraindications to MRI
Sensitivity to gadoliniumPatient's inability to lie prone(Marked kyphosis) Marked obesity Extremely large breastsSevere claustrophobia
Slide28Positron Emission Tomography
It is the most sensitive and specific of all the imaging modalities for breast disease At present, its main use to detect recurrenceAlso useful in multifocal disease, in detecting axillary involvement and in cases of systemic metastases
Slide29• Assist in identification of nonaxillary
lymph node metastasis (ie: internal mammary or supraclavicular lymph nodes) for staging locally advanced and inflammatory breast cancer before starting neoadjuvant therapy •Most expensive and least widely available.
Slide30Thermography
Transmission of heat from the breast, and in malignant lesions results from the hypervascularity Using special heat scanners it is possible to mark “hot” perfusion sites on filmResults are variable and inaccurate, sensitivity is less than 50 percent and it is not advocated as a routine screening method, because it is unable to detect minimal breast cancer.
Slide31FNAC (Fine Needle Aspiration)•Can be done for non-palpable masses
•FNAC takes individual cells
Slide32Tru-cut (Core Biopsy) Needle
Used for:• T≥ 3 cm• operable case
Slide33W.H.O. Classification of Carcinoma of the Breast
Non invasive carcinomaDuctal carcinoma in situLobular carcinoma in situPaget's disease of the nipple (without mass)
Slide34Invasive carcinomaInvasive ductal
carcinoma -- 80%Invasive lobular carcinoma – 10%Mucinous carcinoma -- 2%Medullary carcinoma – 5%Papillary carcinoma -- 1%Tubular carcinoma – 1%Adenoid cystic carcinomaSecretory (juvenile) carcinomaApocrine carcinomaCarcinoma with metaplasia
(
metaplastic carcinoma)Inflammatory carcinoma
Slide35Ductal carcinoma in situ
-originat from terminal duct lobular Units-C\P: mass .pain . discharge-ipsilateral-common(25-70%)
Slide36Slide37Lobular carcinoma insitu
-no clinical sign-no microcalcifictionsby mammogram-bilateral-less(25-35%)
Slide38Invasive ductal carcinomas
• Clinical presentation-Hard, irregular lumpPeau d’orangeInflammation of nippleUlceration of nipple
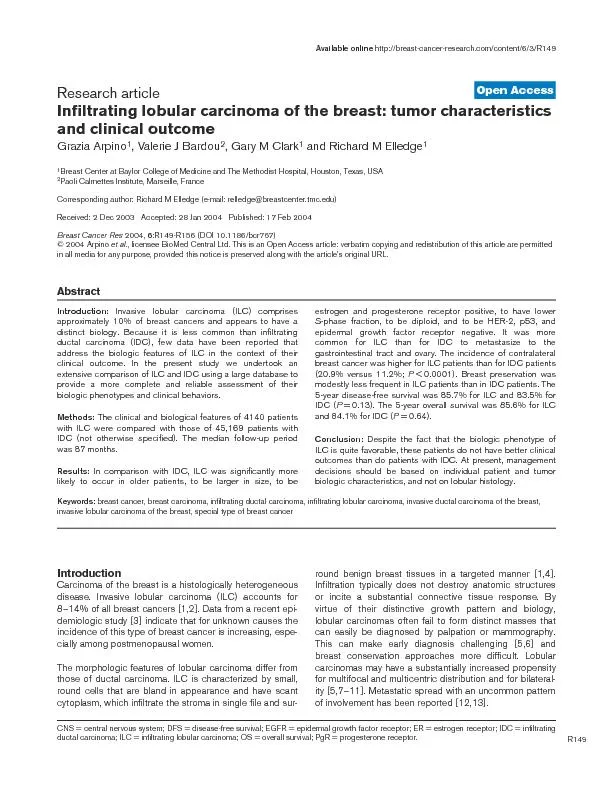
Slide39Invasive lobular carcinoma less common than IDC
C/F:palpable Mass mammographic irregularBordersbilateral and multicentric
Slide40Medullary carcinomas
•common in 6th decadewell- circumsribed mass with rapid growth• 4%• Originates in large ductsthe lesion is deep and mobile.
Slide41Slide42Paget’s disease-Affecting nipple and
areola-Eczema like condition-female>40-1-2%of breast cancer
Slide43Breast mass behind the areola
Hyperplasia of all layersof the epidermis thickening of epidermis followed byulceration of the skin
Slide44Staging: without mass → Stage 0 (carcinoma
insitu) with mass → according to mass sizePrognosis: Good due to:1. Early diagnosis2. Slow rate of growth
Slide45Inflammatory Breast Cancer
Inflammatory breast cancer (IBC) accounts for between 1 percent and 6%The 5-year survival rate for patients with IBC is between 25-50%
Slide46IBC has a high risk of recurrence
Aggressive kind of breast cancerIBC affects women at an average age of 59Black women are more likely than white women
Slide47The Effect of Tumor Size on Survival
Survival
Tumor Size
As tumor size increases, the chance of survival decreases
Slide48Slide49Staging of Breast Cancer•
The American Joint Committee on Cancer(AJCC) has designated staging by TNM• T= tumor size• N = lymph node involvement• M = metastasis
Slide50TNM•
Tx No evidence of primary tumor• Tis Carcinoma in situ• T1 Tumor 2cm or <• T2 2 to 5 cm• T3 T> 5cm• T4a extension to chest wall• T4b edema (including peau d’orange), ulceration of skin, satellite nodules
• T4c T4a + T4b
• T4d Inflammatory carcinoma
Slide51Regional lymph nodes• N0 no regional lymph node metastasis
• N1 Movable ipsilateral axillary lymph node• N2 Fixed ipsilateral axillary lymph n. or internal mammary lymph nodes• N3 -ipsilateral supraclavicular lymph node. -Fixed
ipsilateral
axillary lymph n. and
İnternal
mammary lymph nodes
-
İpsilateral
infraclavicular
lymph node.
Slide52Distant metastasis• M0 - no distant metastasis
• M1 - distant metastasis
Slide53Stage 1• Tumor < 2.0 cm in greatest dimension
• No nodal involvement (N0)• No metastases (M0)• 5-year survival- 87%
Slide54Stage II• Tumor > 2.0 < 5 cm
• Ipsilateral axillary• lymph node (N1)• No Metastasis (M0)• 5-year survival- 75%
Slide55Stage III (Locally advanced)• Tumor > 5 cm (T3)
• or ipsilateral axillary lymph nodes fixed toeach other or other structures (N2)• involvement of ipsilateral internal mammary nodes (N3)• Inflammatory carcinoma (T4d)• 5-year survival- 46%
Slide56Stage IV (Metastatic breast cancer)• Any T
• Any N• Metastasis (M1)• 5-year survival- 13%
Slide57Stage Grouping
Stage 0 Tis
Stage I T1 N0 M0
Stage II T1 N1 M0
T2 N0,1 M0
T3 N0 M0
Stage III Any Worse But M0
Stage IV Any with M1
Slide58SURGICAL
• Radical Mastectomy• Modified RadicalMastectomy• Simple/TotalMastectomy• Breast ConservingSurgery
CHEMOTHERAPY
•
Neo-Adjunctive
Chemotherapy
•
Adjunctive
Chemotherapy
•
Chemotherapy for
Advanced
Metastatic Disease
RADIATION
•
Intra-operative
Irradiation
•
External beam
Radiotherapy
•
Brachytherapy
Slide59SURGERYLumpectomy
Partial or segmental mastectomySimple mastectomyModified radical mastectomySentinel lymph node biopsyAxillary lymph node dissection
Slide60Lumpectomy Surgically removing the
tumor and a smallmargin of healthy tissue around it Followed by radiation therapy May Include removal ofaxillary lymph nodes
Slide61Partial/Segmental MastectomyExcision of mass along with
some portion of breast tissueQuadrantectomy excision of affected quadrant of the breast tissue
Slide62TOTAL/SIMPLE
MASTECTOMY
62
Tissues
removed
:
Tumour,
entire
breast,
areola,
nipple,
skin
over
breast,
Axillary
tail
of
Spence,
Pectoral
fascia
Tissues
retained
:
NO
Axillary
Dissection
Subjected
to
Radiotherapy
later
Slide63Total mastectomy with axillary clearance
63
Common
procedure
Tissues
removed:
Axillary
fat
,
Axillary
fascia
,
Axillary
LN
Slide64Modified Radical mastectomy
Tissues
removed:TM
+
Clearance
of
Axillary
LN
+ Pectoralis
minor
Tissues
preserved
:
Nerve
to
Serratus
anterior,
Nerve
to
Latissimus dorsi,
Intercostobrachial
nerve,
Axillary
Vein,
Cephalic
Vein,
Pectoralis
major
muscle
64
Slide65Sentinel lymph node biopsy:
cancer has spread to the lymph nodes under the arm A blue dye/radioactive substance is injected in orderto identify the sentinel lnwhich drainslymph from the tumor They are then removed.
Slide66 Axillary
lymph node dissectionabout 10 to 40 lymph nodes are removedUsually done at the same time of mastectomy or breast-conserving surgery
Slide67Adjuvant therapy:
After surgeryChemotherapyhormone therapyRadiation therapyNeo-adjuvant therapy:Before surgeryReduce tumorsRadiation therapyChemo therapy
Slide68TreatmentI- Early breast cancer:Non invasive (Stage 0)→ Surgery ± Adjuvant
(postoperative) therapyStage I & II → Surgery + Adjuvant therapy II- Advanced breast cancer:Stage III (Locally advanced) → Neoadjuvant (preoperative) therapy + SurgeryStage IV (Metastatic) → Systemic therapy ± LimitedSurgery
Slide69Early Breast CancerStage I & IISurgery
◦ removing the area of concern and some normaltissue surrounding it is called a lumpectomy◦ removing the breast is called a mastectomy(most women with breast cancer will not need thebreast removed)◦ lymph nodes from under the arm may beremoved with either surgery
Slide70Slide71Early Breast CancerStage I & IIRadiation
Standard treatment after a lumpectomy to reduce the chance of the breast cancer coming back in thesame breastIt is also called local treatment because it affects only the area being treated with radiation
Slide72Slide73Late Breast CancerStage III (Locally Advanced)
First• Neo adjuvant chemotherapy (3-4 cycles) Then• Surgery Then• Post operative chemotherapy (6 cycles) Then• Post operative radiotherapy
Slide74Slide75Late Breast CancerStage IV (Metastatic)
Palliative systemic therapy is the Main line of treatment
Slide76Slide77Breast ReconstructionIntegral part of modern daybreast cancer management
Silicone Implants Lattissimus Dorsi myocutaneous flap Rectus abdominus
myocutaneous flap
Gluteal
Free Flap
Slide78Hormone Treatment◦ growth of many breast
cancers can be blocked bytaking hormone therapy◦Tt is in the form of a pillwhich is taken for 5yrs◦recommended for womenwho have a breast cancerthat is sensitive to hormones
Slide79ER positive disease
PremenopausalTamoxifen for 5 yearsPostmenopausalTamoxifen for 5 yearsfollowed by letrozole
for
5yrsAromatase
inhibitor
(
letrozole
,
anastrozole
,
exemestane
for
5 years)
Slide80Chemotherapy• Treatment with one or more
cytotoxic antineoplastic drugs•Either curative or preventive•Used in conjugation withradiation therapy or surgery• Chemotherapeutic agentsact by killing cells
Slide81Side effects:•
Immunosuppression andMyelosuppression• Gastrointestinal distress• Anemia• Fatigue• Hair loss• Peripheral Neuropathy
Slide82Radiation Therapy• It involves medical use
of ionizing radiation,used in cancer Tt• It can be used as aCurative or adjuvant• Ionizing radiation workby damaging the DNAof cancerous tissuesleading to cellular death
Slide83Side effectsNausea
vomiting LymphedmainfertilityFibrosis of exposed tissueHair lossdryness of mouthDryness of eyes
Slide84Prognosis of breast carcinomas• Major prognostic factors
Tumor Size lymph nodes statusNuclear gradeAgeThe location of the tumor its spread
Slide85“To go fast,
go alone.To go far, go together.”