
One of the important specialized pathways of a number of amino acids is the synthesis of purine and pyrimidine nucleotides These nucleotides are important for a number of reasons Most of them not just ATP are the sources of energy that drive most of our reactions ID: 785057
Download The PPT/PDF document "PURINE METABOLISM AND GOUT" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
PURINE METABOLISM AND GOUT
Slide2One of the important specialized pathways of a number of amino acids is the synthesis of purine and pyrimidine nucleotides.
These nucleotides are important for a number of reasons. Most of them, not just ATP, are the sources of energy that drive most of our reactions.
ATPr
GTP
UTP
AMP
NUCLEOTIDES
Slide3Neither the bases nor the nucleotides are required dietary components.
-We can both synthesize them de novo and salvage and reuse those we already have.
Slide4There are two kinds of nitrogen-containing bases - purines and
pyrimidines
.
Purines
consist of a six-membered and a five-membered nitrogen-containing ring, fused together.
Pyridmidines
have only a six-membered nitrogen-containing ring. There are 4 purines and 4
pyrimidines
that are of concern to us.
Slide5Purines include -
Adenine = 6-amino purine
,
Guanine = 2-amino-6-oxy purine
,
Hypoxanthine = 6-oxy purine
,
Xanthine = 2,6-dioxy purine
Adenine and guanine are found in both DNA and RNA
.
Hypoxanthine
and xanthine are not incorporated into the nucleic acids as they are being synthesized but are important intermediates in the synthesis and degradation of the purine nucleotides.
Slide6Humans catabolize the major purine nucleosides adenosine and
guanosine
to uric acid thus:
Adenosine
Adenosine
Deaminase
Inosine
Purine nucleoside
Phosphorylase Guanosine
Purine Nucleoside Phosphorylase
Xanthine Guanase
Hypoxanthine oxidase Xanthine Guanine Uric acid
Adenosine
Adenosine
deaminase
Inosine
Hypoxanthine
Xanthine
Uric acid
Guanine
Guanosine
Purine nucleoside
phosphorylase
Purine nucleoside
phosphorylase
Xanthine oxidase
Guanase
Xanthine oxidase
Slide7Genetic and Biochemical Basis of
Hyperuricemia
There are at least three different inherited defects that lead to early development of severe
hyperuricemia
and gout:
- Glucose-6-phosphatase
(gene symbol: G6PT) deficiency;
Severe and partial
hypoxanthine-guanine phosphoribosyltransferase (HGPRT, gene symbol: HPRT) deficiency; and elevated 5'-phosphoribosyl-1'-pyrophosphate synthetase (PRPP synthetase
) activity
Slide8DISORDERS OF PURINE METABOLISM
Clinical Disorder
Defective Enzyme
Nature of the Defect
Characteristic of Clinical disorderInheritance patternGout PRPP synthetaseSuperactive (Increased Max)Purine over production and over excretionX-Linked recessiveGoutPRPP synthetaseResistance to feed back inhibitionPurine over production and over excretion
X-Linked recessiveGoutHGPRTase 1Partial deficiencyPurine over production and over excretionX-linked recessiveLesch –
Nyhan SyndromeHGPRTase 1Complete deficiencyPurine over production and over excretion, self mutilation
X-linked recessive
Slide9Von
Gierke’s
disease
In this case purine over production and
hyperuricaemia
(G6P deficiency) occurs secondary to enhanced generation of the PRPP precursor ribose-5-phosphate.
In addition associated lactic acidosis elevates the renal threshold for
urate
elevating total body urates.
Slide10Gout
Gout is a form of inflammatory arthritis characterized by recurrent attacks of a red, tender, hot and swollen joint
.
It is a disorder of purine metabolism and occurs when its final metabolite uric acid crystallizes in the form of monosodium
urate
, precipitating and forming deposits (tophi) in joints, on tendons and in the surrounding tissues.
Slide11Pains typically come on rapidly in less than 12hrs.
The joint at the base of the big toe is affected in about half of cases.
Tophi, kidney stones and
urate
nephropathy, may also result.
Gout occurs due to elevated levels of uric acid in the blood, resulting from a combination of diet and genetic factors.
At high levels, uric acid crystallizes and deposits in joints, and surrounding tissues resulting in an attack of gout
.
Slide12It occurs more commonly in those who eat a lot of meat, drink a lot of beer and are overweight.
Diagnosis may be confirmed by seeing the crystals in joint fluid or tophus.
Blood uric acid levels may be normal during an attack.
Once the acute attack subsides, levels of uric acid can be lowered via life style changes.
Slide13Taking vitamin C and eating a diet high in low fat dairy products may be preventive.
Long standing elevated uric acid levels (
hyperuricaemia
) may result in other symptoms such as hard, painless deposits of uric acid crystal known as tophi (otherwise called crystals of monosodium
urate
).
Extensive tophi may lead to chronic arthritis due to bone erosion.
Hyperuricaemia
may also result in uric acid stones precipitating in the kidneys resulting in urate nephropathy.
Slide14CAUSES OF GOUT
Diet / lifestyle
accounts for about10 to 12% of cases of gout and is associated with, alcohol, fructose sweetened drinks, meat and seafood, also physical trauma and Surgery.
Consumption of coffee, vitamin C and dairy products as well as physical fitness, appear to decrease the risk.
Genetic predisposition
contributes to about 60% of variability in uric acid level. Mutations in certain genes related to
urate
metabolism can lead to increased risk of hyperuricaemia and gout.
Slide15Medical Conditions
- Metabolic syndrome (a combination of abdominal obesity, hypertension, insulin resistance and abnormal lipid levels, occurs in about 75% of cases), other conditions complicated by gout include lead poisoning, kidney failure, hemolytic anemia, psoriasis, solid organ transplants ,
leukaemia
(especially acute
leukaemia
during treatment), starvation,
myeloproliferative
disorders example polycythemia.
Chronic lead exposure is a risk factor for gout due to the harmful effect of lead on kidney function.Lesch – Nyhan syndrome is often associated with gouty arthritis.
Slide16MEDICATION
Diuretics
Niacin
Aspirin
ACE inhibitors
Angiotensin receptor blockers (except losartan)
Beta blockers
etcetera all tend to precipitate gout.
Slide17Under excretion of
urate
is the primary cause of
hyperuricaemia
in about 90% of cases.
Over production is the cause in less than 10%
The risk of developing Gout depends on the degree of
hyperuricaemia
. When levels are between 415 and 530 µmol/l (7 and 8.9g/dl), The risk is 0.5% /year, while in those with a level greater than 535 µmol/l (9mg/dl), the risk is 4.5% / year. Reference range of uric acid – male- 3.4 – 7.2 mg/dl (200 – 430 micromole/L). Female- 2.4 – 6.1 mg/dl (140 – 360 micro mole/L)
Slide18PATHOPHYSIOLOGY
The triggers for precipitation of uric acid are not well understood.
It may precipitate at normal levels.
But it is more likely to do as levels increase
Other triggers include cool temperature, acidosis, extra cellular matrix proteins such as proteoglycans, collagens and chondroitin sulfate.
Slide19DIAGNOSIS
If one has
hyperuricaemia
and the classic acute arthritis of the base of the great toe (known as
podogra
) there may not be any used for further investigations to diagnose gout in the patient.
Synovial fluid analysis (Identification of Monosodium
urate
crystals in S.F or a tophus) SF is obtained by arthrocentesis.
Slide20Blood tests –
inc
(a) plasma uric acid level.
Hyperuricaemia
is defined as a plasma
urate
level greater than 420 µ
mol
/l (7.0 mg/dl) in males and 360 µmol/l (6.0 mg/dl) in females.- WBC counts- Kidney function
Slide21- urine uric acid test (secondary test , to evaluate whether the kidneys are excreting enough uric acid) kidneys filter uric acid out of the blood stream and dispose of it through the urine.
- If the kidneys are unable to do this well, uric acid accumulates in the blood, leading to elevated blood uric acid levels.
Slide22DIFFERENTIAL DIAGNOSIS
The most important differential diagnosis in gout is septic arthritis which should be considered in those with signs of infection or those who do not improve with treatment.
Here a synovial fluid Gram stain and culture may be performed.
Other similar conditions include
psendogout
, rheumatoid arthritis, psoriatic arthritis and reactive arthritis.
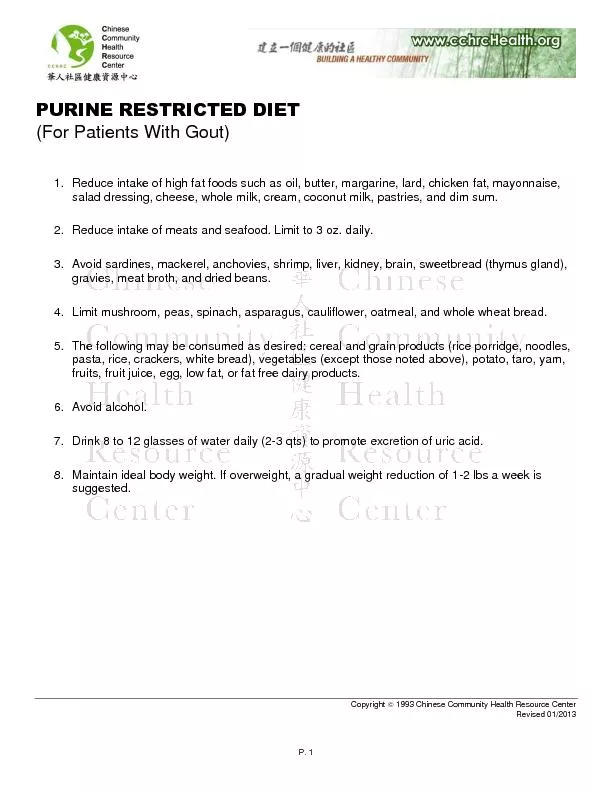
Slide23Prevention can be achieved by
Life style changes especially as it concerns dietary changes including reducing intake of purine rich foods of animal origin e.g. meat, seafood, alcohol, fructose (especially high fructose corn syrup) and switching to dairy prods, vitamin C, coffee and cherries may help prevent gout, also losing weight.
Gout may be secondary to sleep apnea via the release of purines from oxygen starved cells. Treatment of apnea can lessen the occurrence of attacks.
Medication can also decrease uric acid levels.
Slide24TREATMENT
Aim to settle the symptoms of an acute attack.
Repeated attacks can be prevented by medications that reduce serum uric acid levels.
Drugs include – NSAIDS, colchicine, and steroids.
Options for prevention / prophylaxis include
Allopurinol,
febuxostat
and
probenecid.
Slide25