PDF-Article published online 20210802
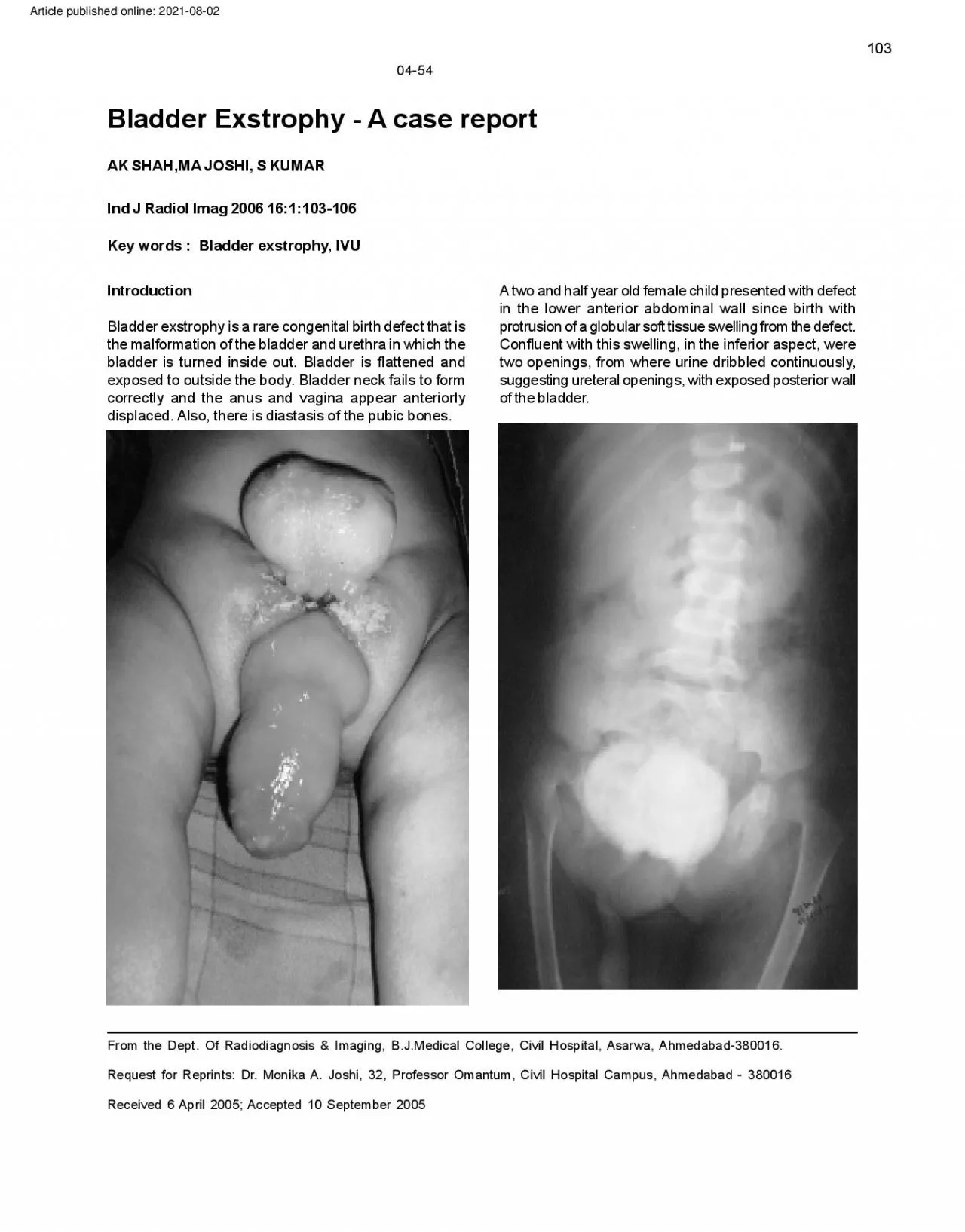
103 0454 Bladder Exstrophy A case report AK SHAHMA JOSHI S KUMAR Ind J Radiol Imag 2006 161103106 Key words Bladder exstrophy IVU Introduction A two and half year
Download Presentation
"Article published online 20210802" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement.
Presentation Transcript
Transcript not available.