PDF-CENTER FOR DRUG EVALUATION AND RESEARCHAPPLICATION NUMBER:205858Orig1s
Author : cheryl-pisano | Published Date : 2016-04-27
OFFICE DIRECTOR MEMO Office Director Summary Review NDA 205858 Zydelig idelalisib On September 11 2013 Gilead Sciences Inc submitted an NDA for Zydelig idelalisib
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "CENTER FOR DRUG EVALUATION AND RESEARCHA..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
CENTER FOR DRUG EVALUATION AND RESEARCHAPPLICATION NUMBER:205858Orig1s: Transcript
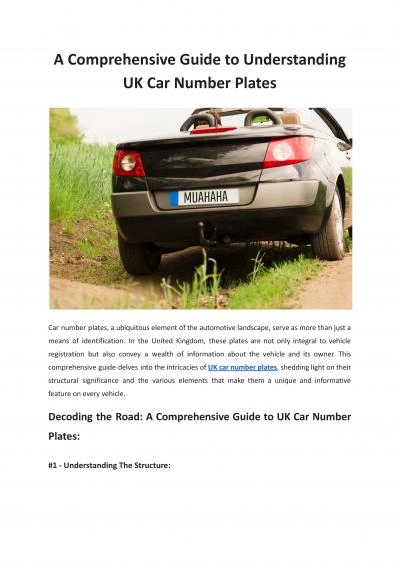
OFFICE DIRECTOR MEMO Office Director Summary Review NDA 205858 Zydelig idelalisib On September 11 2013 Gilead Sciences Inc submitted an NDA for Zydelig idelalisib for the proposed indication. DFXED LYLVLRQ57347RI57347DVWURHQWHURORJ DQG57347QERUQ57347UURU 3URGXFWV LFKDUG5734757355HV5735657347VKLKDUD ULDQ573476W URQJLQ LYLVLRQ57347RI 3XOPRQDU OOHUJ 5735957347DQG573475KHXPDWRORJ 3URGXFWV 6DQG57347DUQHV LYLVLRQ57347RI573470HWDEROLVP57347DQ 6 POLICY AND PROCEDURES OFFICE OF NEW DRUGS Good Review Practice Management of Breakthrough TherapyDesignated Drugs and Biologics Table of Contents PURPOSE 1 BACKGROUND Learning objectives. By the end of this presentation, you will be able to:. Explain evaluation design . Describe . the differences between types of evaluation . designs. Identify . the key . elements . Reclaiming Futures/Juvenile Drug Court Evaluation. Josephine Korchmaros, PhD. Southwest Institute for Research on Women. University of Arizona. National Association of Drug Court Professionals Conference . Program Evaluation Webinar Series Part 1: “Top Roadblocks on the Path to Good Evaluation– And How to Avoid Them” Presented by: Tom Chapel Top Roadblocks on the Path to Good Evaluation– And How to Avoid Them . SYFTET. Göteborgs universitet ska skapa en modern, lättanvänd och . effektiv webbmiljö med fokus på användarnas förväntningar.. 1. ETT UNIVERSITET – EN GEMENSAM WEBB. Innehåll som är intressant för de prioriterade målgrupperna samlas på ett ställe till exempel:. Christine Murray, UNC Greensboro. Cindy . Fraga Rizo, . UNC Chapel Hill. Tonya VanDeinse, UNC Chapel Hill. Presentation Overview. Data & Evaluation Strategies of the Guilford County Family Justice Center – . Pima County Reentry Center (PRC). Pima County Adult Detention Center (PCADC) . CMS Southern AZ Correctional Health Programs. Medication Assisted Treatment – Prescription Drug & Opioid Addiction (MAT PDOA) Program. NDA 206353 ATV/COBI FDC CDTL Review mentioned phase III trialand a phase IItrialTrialGS-US-216-0105 as reviewed in NDA The findings of this study was extrapolatedto HIV-1treatment-experienced patients For more information about the New York Advanced Headache Center, our doctors, or to schedule a consultation with Amr Hosny MD, please contact our headache, migraine specialists in New York City by number: 646-763-2222. Additional copies are available from: Office of Communications, Division of Drug Information Center for Drug Evaluation and Research Food and Drug Administration 10001 New Hampshire Ave., Hillandale B Travis R. . Goodwin. 1. , . Dina . Demner-Fushman. 1. , Kin Wah Fung. 1. , . and . Phong. Do. 2. 1. . Lister Hill National Center for Biomedical Communications, . U.S. National Library of Medicine. This comprehensive guide delves into the intricacies of UK car number plates, shedding light on their structural significance and the various elements that make them a unique and informative feature on every vehicle. Experience the best eye care center in Pune. The best clinics for your eye health, include the prestigious Dr. Sonalika Eye Clinic. At Hadapsar, Amanora, Magarpatta, Mundhwa, Kharadi Rd, Viman Nagar, Wagholi, and Wadgaon Sheri
Download Rules Of Document
"CENTER FOR DRUG EVALUATION AND RESEARCHAPPLICATION NUMBER:205858Orig1s"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents