PDF-Inscribing behaviour in information infrastructure standardsNR, PB 114
Author : conchita-marotz | Published Date : 2016-04-28
1 2 and brie
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Inscribing behaviour in information infr..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Inscribing behaviour in information infrastructure standardsNR, PB 114: Transcript
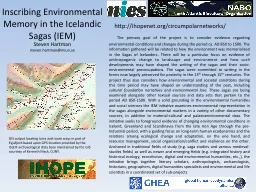
1 2 and brie. " on the Marine Corps homepage at http://www.usmc.mil Current Award, Campaign, Service, and Expeditionary Stre1. Presidential Unit Citation (Navy) Streamer with six silver and three bronze stars 2. Pr Diagnosis, Definition, . Bias. Explanations. Treatments. HEALTH & CLINICAL PSYCHOLOGY . G543. Diagnosis. : DSM & ICD . Definitions . of . Abnormality: . Rosenhan. & Seligman). Bias: . Ford & . 1. PPT-114-01. There are over 3,000 species of snakes.. Every year there are nearly 7,000 snake bites.. Snake’s . scales are made up of . Keratin. , which is the same thing that our fingernails are made from. Musculoskeletal problems in bricklayers, Adele Reid, Andrew Pinder and Simon MonningtonDr ADJ Pinder 1.To carry out a comprehensive literature review of epidemiological and ergonomicstudies of muscul Captivity, Return, and Years of Silence. Lesson . 16: The Prophet Malachi (Pg. 110-114). 612 B.C.. 606 B.C.. 586 B.C.. 539 B.C.. 536 B.C.. 520 B.C.. 516 B.C.. 483 B.C.. 458 B.C.. 445 B.C.. 430 . B.C.. SERAPHIC PLANETARY GOVERNMENT. Paper 114 - Video study group link part 1. Paper113 - Seraphic Gaurdians of Destiny. Paper 114 - Video study group link part . 2. We would like to give a special thanks to Don Estes for the use of the information from his Chart The Origin, History and Destiny of Universe Reality. We would also like to thank the creator of . SERAPHIC PLANETARY GOVERNMENT. Paper113 - Seraphic Gaurdians of Destiny. Paper 114. Seraphic Planetary Government. Audio . Version. (1250.1). . 114:0.1. The . Most Highs. rule in the kingdoms of men through many celestial forces and agencies but chiefly through the ministry of . Core_114_AS_July 2013. Module :Objectives. Participants are able to:. Defend and compare the concepts of safe and unsafe.. Illustrate and justify the application of the danger threshold.. Evaluate family conditions as danger threats utilizing the danger threshold.. 1. PHY 114 A General Physics II. 11 AM-12:15 . P. M TR Olin 101. Plan for Lecture 1:. Welcome . & overview. Class structure & announcements. Electrical . charges and forces. 1/18/2012. PHY 114 A Spring 2012 -- Lecture 1. There are over 3,000 species of snakes.. Every year there are nearly 7,000 snake bites.. Snake’s . scales are made up of . Keratin. , which is the same thing that our fingernails are made from. .. The Hognose, Grass snake and the Spitting Cobra will fake death when feeling threatened. They . Steven Hartman. steven.hartman. @. miun.se. . The primary goal of the project is to consider evidence regarding environmental conditions and changes during the period ca. AD 850 to 1500. The information gathered will be related to how the environment was memorialized in the Sagas of Icelanders. There will be a particular focus on evidence of anthropogenic change to landscape and environment and how such developments may have shaped the writing of the sagas and their socio-environmental preoccupations. The sagas were committed to writing in the forms now largely preserved for posterity in the 13. ECM01F State ENG Rev 11 / 18 - D www. - Topics/ENE - ECM.aspx #tab05Provider Page 1 of 1 State of Minnesota District Court County Judicial District: Court File Number: Case Type: Financial Ear VerDate 11-MAY-200020:01 Jan 05, 2001Jkt 089139PO 00523Frm 00002Fmt 6580Sfmt 6581E:\PUBLAW\PUBL523.106APPS24PsN: PUBL523 VerDate 11-MAY-200023:50 Dec 20, 2000Jkt 089139PO 00523Frm 00003Fmt 6580Sfmt 65 ). Department of Oral and Maxillofacial Surgery. Gullas Medical Center. University of the Visayas, Philippines. Conservative protocol . for . Ameloblastoma. Standard treatment modalities. Cystic. Enucleation + modalities .
Download Document
Here is the link to download the presentation.
"Inscribing behaviour in information infrastructure standardsNR, PB 114"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents