PPT-Washington Association of Medical Staff Services
Author : danika-pritchard | Published Date : 2018-03-15
Presented by Eric J Neiman and Sharon C Peters Resolving Disputes in the Credentialing and Privileged World Credentialing and Privileging Goal for both is quality
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Washington Association of Medical Staff ..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Washington Association of Medical Staff Services: Transcript
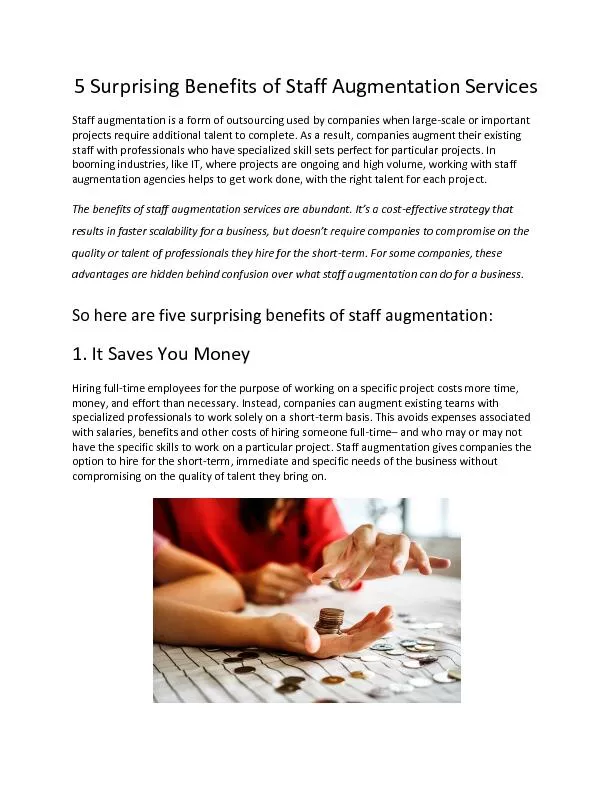
Presented by Eric J Neiman and Sharon C Peters Resolving Disputes in the Credentialing and Privileged World Credentialing and Privileging Goal for both is quality and safety Credentialing verifies whether provider meets certain criteria relating to professional competence and conduct. Professor Peter Swire. Ohio State University. Privacy Working Group. April 25, 2012 . Overview. Linguistics: “network” and “association”. Social networks as platforms for association. Cyber conferences. Professor Steve Thornton, Dean. July 2 2014. Mission statement. To . improve Health in the South West and beyond. Prevention. Treatment. World Class Research. Top quality Education . (Scientists, Doctors, Radiographers). Health Insurance Exchange. Phil Dyer. Board Member. Disclaimer;. The views and information expressed are my personal opinions and perspectives and do not represent the official position of the State of Washington or the Washington State Health Insurance Exchange Board or Staff.. April 2014. . . About CAMP . CAMP represents 30+ of Canada’s most influential medical journal/publication brands. Collectively our publications saturate the market with . content including research. Safe Deliveries Roadmap. On-Boarding Webcast . June 13, 2013. Presented at Washington State Hospital Association Safe Table, 6/13/13. Safe Deliveries Roadmap Project Coordinator. Mara . Zabari. , Director of Integration Partnership for Patients. A “new” network led by the Washington Invasive Species Council and partners with the goal of harmonizing messaging, resources, and reporting pathways between existing programs. .. Goal. NOT to actively search for invasive species. EASTERN WASHINGTON UNIVERSITY. THE EVERGREEN STATE COLLEGE. UNIVERSITY OF WASHINGTON. WASHINGTON STATE UNIVERSITY. WESTERN WASHINGTON UNIVERSITY. October 2016. Paul Francis. Executive Director. About COP. Learning Objectives. Examine and discuss beliefs about personal and professional ethics. Identify how your beliefs and values affect your daily decisions. Discuss NAMSS Ethics Policies and the NAMSS Code of Conduct. Staff augmentation is a form of outsourcing used by companies when large-scale or important projects require additional talent to complete.
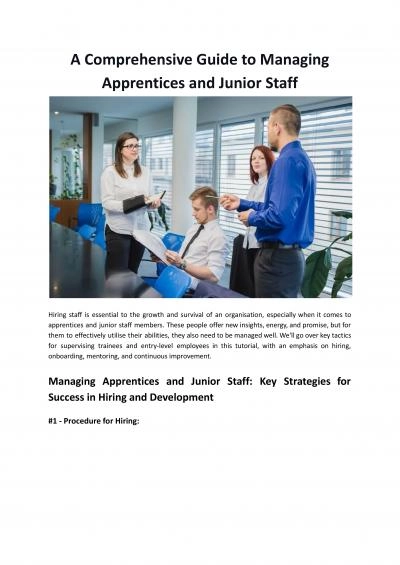
https://www.elevano.com/5-surprising-benefits-of-staff-augmentation-services/ Use our guide to find all of the supported exchanges and bitcoin ATMs within Washington quickly and efficiently. Download it now. Visit: https://www.smartbitcoininvestments.com/buy-bitcoin-in-washington/ SubjectAmendmentto E-8061 Gifts to Physicians from IndustryPresented by Susan Dorr Goold MD Chair Referred to Reference Committee on Amendments to Constitution and BylawsLarry E ReavesMD ChairOpinion 40 Years of Service to the FieldPrepared by Hunter R Boylan PhD January 2000Revised January 2001 December 2003 January 2005 February 2010 January 2012 January 2013 December 2014 and February 2016----- Your Department Name Overview. Reporting Structure and Staffing. Interactions with Your Organizations Name At large. Scope of Services. Credential / Privileging Primer. Your Departments Structure . and Staffing. Explore key tactics for trainees and junior staff with an emphasis on hiring, onboarding, mentoring, and continuous improvement.
https://staffflex.co.uk/comprehensive-guide-to-managing-apprentices-junior-staff/
Download Document
Here is the link to download the presentation.
"Washington Association of Medical Staff Services"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents