PDF-Middle East respiratory syndrome coronavirus (MERS-CoV) in dromedary c
Author : luanne-stotts | Published Date : 2016-05-30
1 R wwweurosurveillanceorg 2 gene region 11 and by five other RTPCRs designed for subsequent phylogenetic analysis Table The MERSCoV genome organisation and the
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Middle East respiratory syndrome coronav..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Middle East respiratory syndrome coronavirus (MERS-CoV) in dromedary c: Transcript
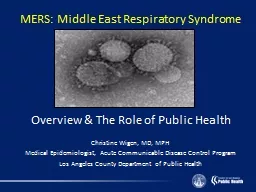
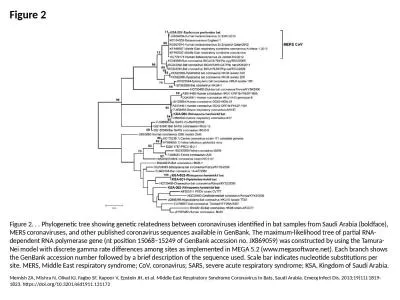
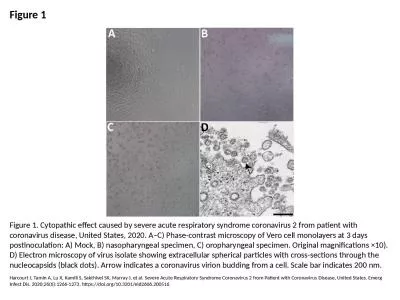
1 R wwweurosurveillanceorg 2 gene region 11 and by five other RTPCRs designed for subsequent phylogenetic analysis Table The MERSCoV genome organisation and the location of. Author af�liations: Netherlands Centre for Infectious Disease Control, Bilthoven, the Netherlands (C.B.E.M. Reusken, G.-J. Godeke, I. Zutt, M.P.G. Koopmans); Erasmus Medical Center, Rotterd (MIR . ee. . ud. ) – an extremely large number 1. Steve said she had a MYRIAD of things to do to get ready for the party.. 2. On a clear night in Alaska the sky is filled with a MYRIAD of stars.. C. o. V. . (Middle East R. espiratory. . Syndrome-Co. ronavirus). Oregon Society for Respiratory Ca. re Annual Conference. March 2, 201. 6. Carl Eckrode, Ph.D., . MPH, RRT. OverVIEW. Background-The History of MERS. Overview & The Role of Public Health. Christine Wigen, MD, MPH. Medical Epidemiologist, Acute Communicable Disease Control Program. Los Angeles County Department of Public Health. THANK YOU. LAC DPH. Local Health Department Nurses Meeting. August 15, 2013. T.J. Sugg, MPH. Objectives. Introduce new regional epidemiologists. Staffing changes on the Reportable Diseases Section. Highlight changes to MERS-. What are coronaviruses and MERS-co? Where did it come from and how has it evolved? What clinical and evolution can we expect? What do we know about transmisibility? How will we treat it? . 4. th. Example of Human Specific Disease:. . Coronaviruses. . Classification. . morphology and structure.. . Laboratory diagnosis.. . Treatment and Prevention. What are Coronaviruses?. CTropMed. 3/17/20. COVID-19. SARS-CoV-2. 2019-nCov. HCoV-19. Disease. Virus Name. 7 Human Coronaviruses:. 4 normal; 3 “novel”. Alpha: . HCoV-229E. , . HCoV-NL63 . Beta: . HCoV-HKU1. , . HCoV-OC43. May 27. 2020. K.Dharmalingam. Asymptomatic Likely but remote. Prodromal Yes. Oligosymptomatic Yes. Polysymptomatic Yes. Spread occurs from all these groups of patients. Fauci. , for one, still believes it does.. Analytical & Clinical Performance Data (OUS). June 2020. HOOD05162003091712. FTD SARS-CoV-2 Assay*. Instructions for Use. *. CE-IVD labelled for diagnostic use in the EU. . The . Instructions for Use . 2019). PRESENTED BY. Image: . “Coronaviruses viewed under an electron microscope. Note the characteristic crown-like (corona) appearance” . By CDC/Dr. Fred Murphy. ETIOLOGY. Coronaviruses (. CoV. 234 elds. As of 31 January 2018, a total of 221 articles were retrieved, and 216 of them were written in English. The full texts of the English articles were reviewed and crit - ically assessed Memish ZA, Mishra N, Olival KJ, Fagbo SF, Kapoor V, Epstein JH, et al. Middle East Respiratory Syndrome Coronavirus in Bats, Saudi Arabia. Emerg Infect Dis. 2013;19(11):1819-1823. https://doi.org/10.3201/eid1911.131172. Harcourt J, Tamin A, Lu X, Kamili S, Sakthivel SK, Murray J, et al. Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States. Emerg Infect Dis. 2020;26(6):1266-1273. https://doi.org/10.3201/eid2606.200516.
Download Document
Here is the link to download the presentation.
"Middle East respiratory syndrome coronavirus (MERS-CoV) in dromedary c"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents