PDF-Mechanical Ventilation Guidelines
P5
STICU
BICU
I
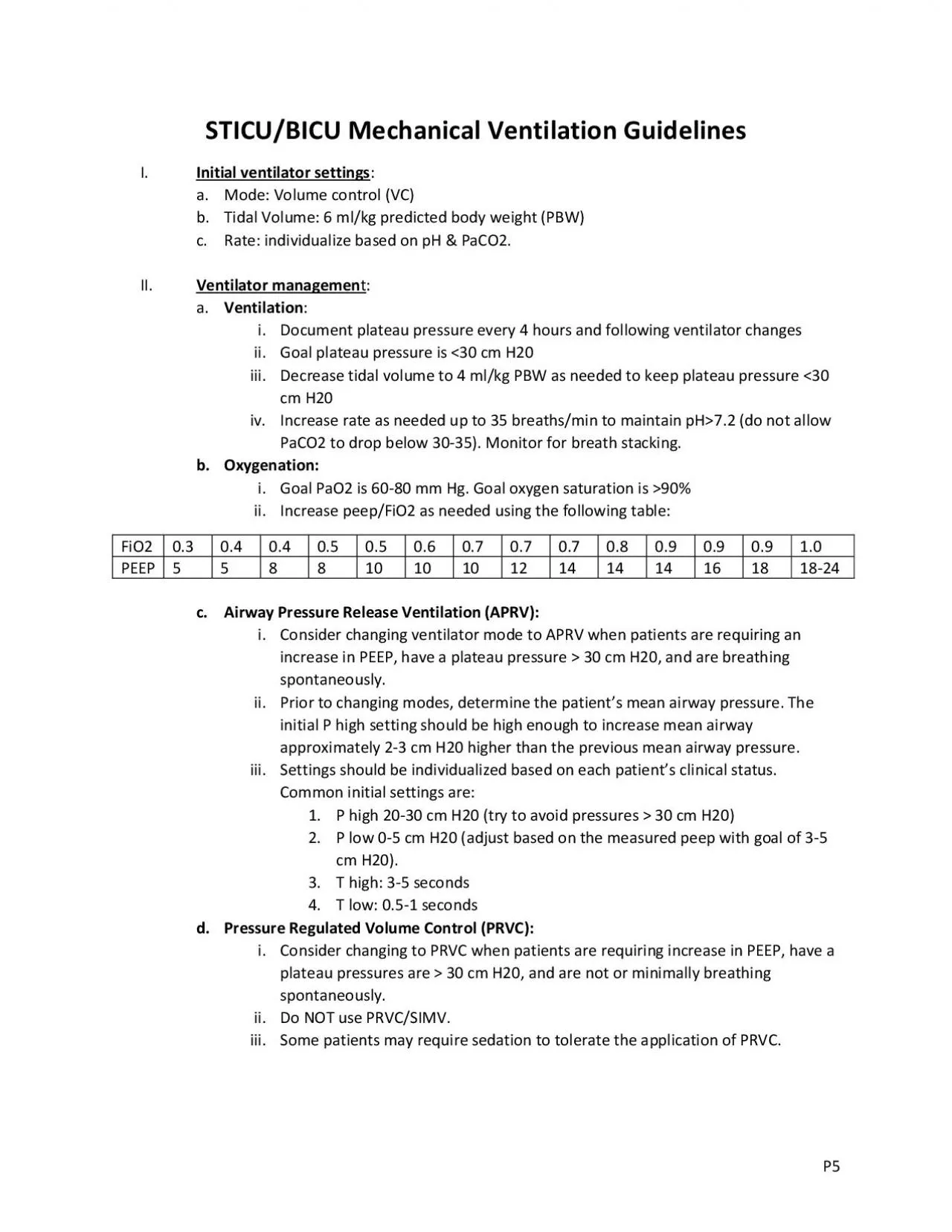
Initial ventilator settings a
Mode Volume control VC
b
Tidal Volume 6 mlkg predicted body weight PBW c
Rate individualize based on pH PaCO2 II
Ventilator
Download Presentation
"Mechanical Ventilation Guidelines" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement.
Presentation Transcript
Transcript not available.