PDF-Transfer of Care
Author : myesha-ticknor | Published Date : 2016-11-17
Monthly Delayed S it R e p s D efinitions and g u idance V ersion 10 8 Monthly Delayed Transfer of Care SitReps Definitions and Guidance 2 Version control Version Date
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Transfer of Care" is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Transfer of Care: Transcript
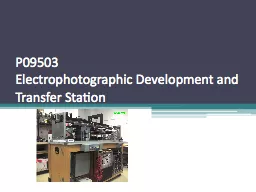
Monthly Delayed S it R e p s D efinitions and g u idance V ersion 10 8 Monthly Delayed Transfer of Care SitReps Definitions and Guidance 2 Version control Version Date issued Changes made 100 18. 4Life Center are independent 4Life distributors of 4Life Transfer Factor and other 4Life supplements. At 4Life Center, we offer 4Life Transfer Factor at wholesale prices, so you don’t have to break the bank in order to make great improvements to your health. Strong academic preparation and performance are primary elements in our admission decisions The average GPA of transfer applicants who are admitted to UCLA is more than 35 and most students who are admitted have completed most or all of the preparat Handbook for the Oil . & Gas Industry. August 2012. All materials, content and forms contained in this handbook are the intellectual property of TPA, and may not be copied, reproduced, distributed or displayed without TPA's express written permission.. Created By: Haley . Vrazel. . Objectives. Analyze . in great depth embryo . transfer. List and describe the . steps . of embryo . transfer. Compare and Contrast AI with . ET. Argue the pros and cons of . Heat Transfer . is the transport of . thermal energy. due to a temperature difference across a . medium(s. ). mediums: gas, liquid, solid, liquid-gas, solid-gas, solid-liquid, solid-solid, etc.. Thermal Energy. This case of heat transfer happens in different situations.. It is complicated process occupies an important side in applied mathematics to find a solution for Fourier’s low as a partial differential . Sara Duclos, Kayla Eckley, Joseph McGrath, Department of Chemical Engineering, University of New Hampshire. Introduction. Objectives. Methods. Results. Design Problem. References. Condensers are involved within systems in order to cool an environment with the evaporation and condensation of a fluid. Presentation for NACADA Salt Lake City National 2013. by. Dena Ford, Ryan Sexton, and Chauntrice Riley. College of Sciences. University of Central Florida. Presentation Objectives. Provide motivation for institutional modification of a long-held schedule. Lecture slides by. Mehmet . Kanoglu. Copyright © The McGraw-Hill Education. Permission required for reproduction or display.. Thermodynamics: An Engineering Approach . 8th . Edition. Yunus A. . Ç. engel, Michael A. Boles. Team Members. Name. Discipline. David Schwartz. ISE. Ruth Gay. ME. Phillip Lopez. ME. Dan Summers. ME. Rachel Chrash. EE. Min-Shi Hsiao. EE. Andrew Kearns. EE. Sasha Oliver. CE. Project Description. The purpose of this project is to make an existing electrophotographic development and transfer station functional and to improve the usability, safety and sensing abilities. . Five Key Initiatives. Office of Transfer Articulation - . Jane Rex. Jump Start Appalachian . – Phil Lewis. Transfer Pre-Orientation Program . – Phil Lewis. Transfer Services Team . – Phil Lewis. Looking for facility based residential care homes in the UK? Connect with Minster Care Group that provides amazing nursing care services for elderly. Jamila C. Pollard, Esq.. Program Manager Senior/Legal Officer. Family Engagement and Dispute Resolution. Division for Special Education Services and Supports. Learning Targets. I can explain to parents and students the IDEA’s transfer of rights provision.. Experience the best eye care center in Pune. The best clinics for your eye health, include the prestigious Dr. Sonalika Eye Clinic. At Hadapsar, Amanora, Magarpatta, Mundhwa, Kharadi Rd, Viman Nagar, Wagholi, and Wadgaon Sheri
Download Document
Here is the link to download the presentation.
"Transfer of Care"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents