PPT-The rhrumatological lectures schedule for 5
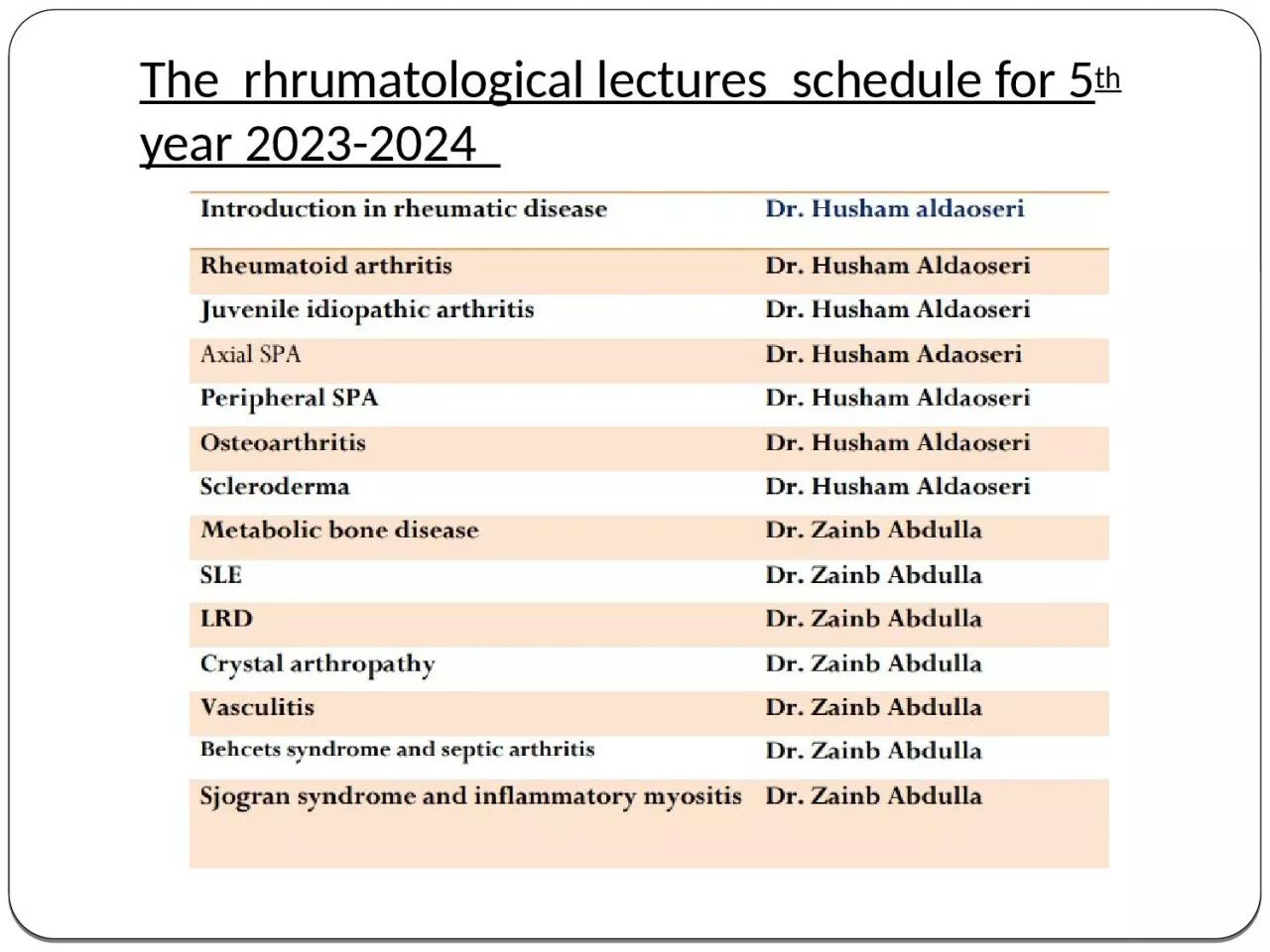
th year 20232024 INTRODUCTION TO RHEUMATOLOGY What is Rheumatology A medical science devoted to the study of rheumatic diseases and musculoskeletal disorders Approximately
Download Presentation
"The rhrumatological lectures schedule for 5" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement. Download
Presentation Transcript
Transcript not available.