PDF-OILGAS LEASE OPERATOR AND NONOPERATOR SUPPLEMENTAL
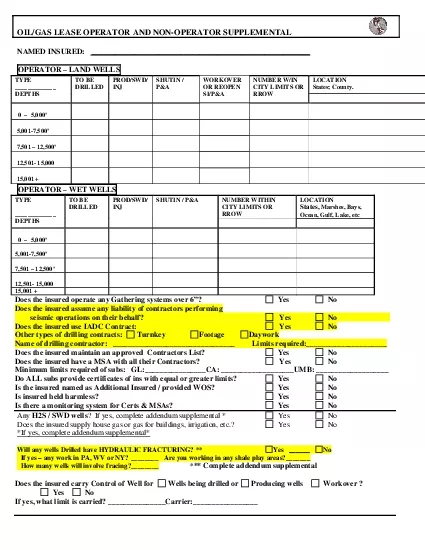
NAMED INSURED OPERATORLANDWELLSTYPE DEPTHSTO BE DRILLEDPRODSWDINJ SHUTIN PAWORKOVEROR REOPENSIPANUMBER WIN CITY LIMITS OR RROWLOCATION States County5000146500175001467501
Download Presentation
"OILGAS LEASE OPERATOR AND NONOPERATOR SUPPLEMENTAL" is the property of its rightful owner. Permission is granted to download and print materials on this website for personal, non-commercial use only, provided you retain all copyright notices. By downloading content from our website, you accept the terms of this agreement.
Presentation Transcript
Transcript not available.