PDF-Name of Healthcare Facility ReceivingRequesting Funding Street Address City State Zip
Author : tatyana-admore | Published Date : 2015-02-20
S Department of Health Human Services Office for Civil Rights 200 Independence Ave SW Washington DC 20201 Name and Title of Authorized Official please print or type
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Name of Healthcare Facility ReceivingReq..." is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Name of Healthcare Facility ReceivingRequesting Funding Street Address City State Zip: Transcript
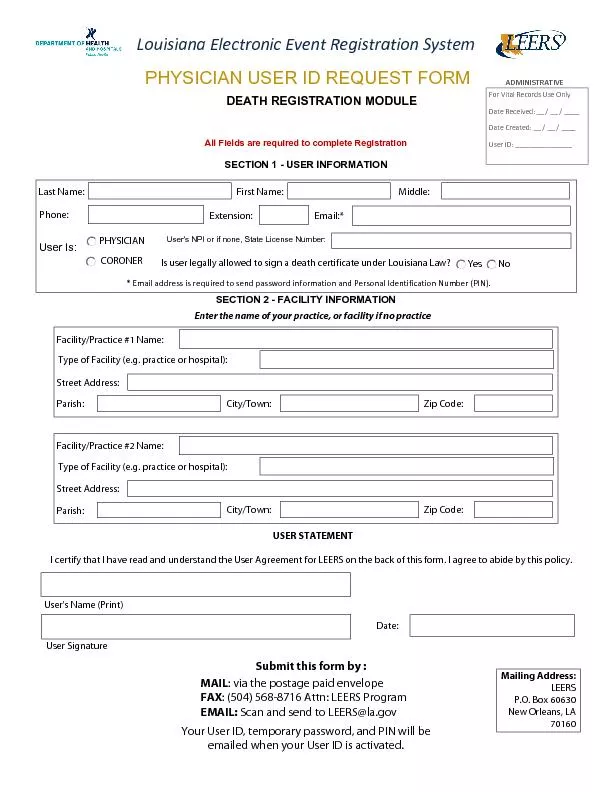
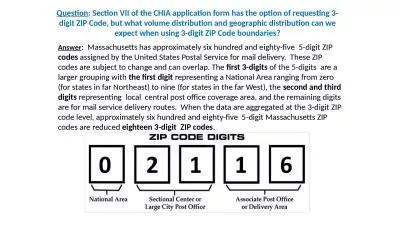
S Department of Health Human Services Office for Civil Rights 200 Independence Ave SW Washington DC 20201 Name and Title of Authorized Official please print or type ASSURANCE OF COMPLIANCE ASSURANCE OF COMPLIANCE WITH TITLE VI OF THE CIVIL RIGHTS AC. Party Host Host ess Merchandise Arcade Food Concessions Park Services Janitorial Petting Zoo Guest Relations Front Desk Stage Theater Ride Operator must be 18 1 2 3 AFTER listing your job preferences you can select Any department to inc However if demand for bowl tickets exceeds the allocated amount there will be a limit placed on the number of tickets that can be purchased Please visit okstatepossecombenefits for bowl ticket limits Seat locations and price levels are determined by On January 1 was any portion of this property used for commercial purposes or rented to another person or entity for more than 6 months Yes No Check your type of residence Singlefamily dwelling Duplex Townhouse Condominium Apartment Other Yes No On Use a separate form for each individual puchasing a Climbing Pass Type your information in the fields below print out the completed form and sign it If returning the form by mail send it to Mount Rainier National Park Wilderness Information Center 5 7336315 370 A57577ropostale 7207336795 325 ALDO 7207336179 600 American Eagle Out64257tters 3036633904 185 Ann Taylor Factory Store 3036883335 670 ArcTeryx 3035865567 830 SICS Outlet 3036888699 802 Banana Republic Factory Outlet 3036889116 340 GH Bas On January 1 was any portion of this property used for commercial purposes or rented to another person or entity for more than 6 months Yes No Check your type of residence Singlefamily dwelling Duplex Townhouse Condominium Apartment Other Yes No On http://www.buyziplinekitsnow.com buyziplinekitsnow offer the best cheap zip lines for home and the most reliable and affordable zip line cable and harnesses for kids and adults. Our best affordable most inexpensive zip line trolleys will make your backyard garden home zip line provide you with years of fun, memorable experiences. Intent to Apply for Financial Aid and Complete the FAFSA Form Bunker Hill Community College awards millions of dollars in federal state and institutional fi nancial aid each year to eligible students However many students miss out because they do no Street Address: Zip Code: City/Town: Parish: Facility/Practice #2 Name: Louisiana Electronic Event Registration SystemPHYSICIAN USER ID REQUEST FORM For Vital Records Use OnlyDate Received: __ / __ / for a reimbursement payment.. 1. This form is only used after a club member has purchased supplies with their personal funds instead of the club’s budget. . This should be a last resort option. . We will not reimburse 1 student for large amounts of money. . VP012 (Rev) APPLICATION FOR DUPLICATE NEVADA CERTIFICATE OF TITLE NSTRUCTIONS– PLEASE READ CAREFULLYIf an original Nevada Certificate of Title has been lost, stolen, or mutilated, a duplicate ti Page 1 of 1 S Statement of Information (Domestic Stock and Agricultural Cooperative Corporations) If this is an amendment, see instructions. IMPORTANT – READ INSTRUCTIONS BEFORE COMPLETING THIS Description and Volume of Rejected WastePMAMWaste Generation Site/Location Time of Waste RejectionSignatureZIP CodeFacility NameStateCityAddressWHERE THE WASTE WAS FINALLY DISPOSEDE-mail AddressZIP Co Answer. : Massachusetts has approximately six hundred and eighty-five 5-digit ZIP . codes . assigned by the United States Postal Service for mail delivery. These ZIP codes are subject to change and can overlap. The .
Download Document
Here is the link to download the presentation.
"Name of Healthcare Facility ReceivingRequesting Funding Street Address City State Zip"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents